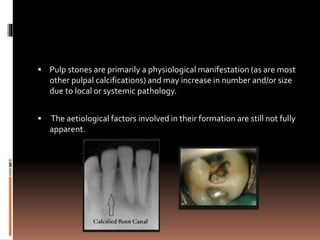
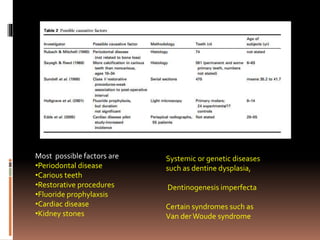
This document discusses pulp calcification and pulp stones. It notes that pulp stones are a physiological manifestation that may increase in number or size due to local or systemic pathology. The etiological factors involved in their formation are not fully understood. As people age, the pulp space decreases in size and the blood vessels, nerves, and cells in the pulp also decrease. Pulp stones can form due to factors like age, circulatory disturbances, orthodontic tooth movement, and genetic predisposition. They are typically composed of calcium and phosphorus. Pulp stones may block access to canal orifices or engage instruments, but can usually be removed during root canal treatment with magnification, access, and proper instruments.






































![Age changes in enamel, dentin and pulp1 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/agechangesinenameldentinandpulp1autosaved-240807163606-82ece9c9-thumbnail.jpg?width=640&height=640&fit=bounds)


















































