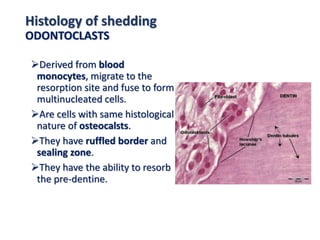
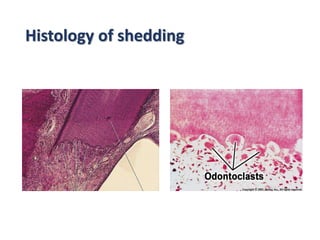
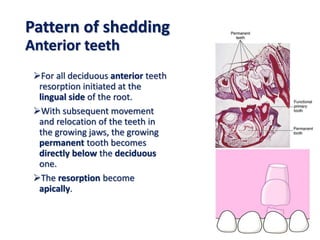
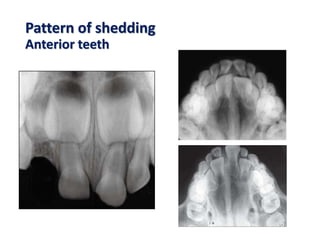
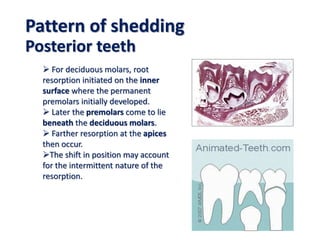
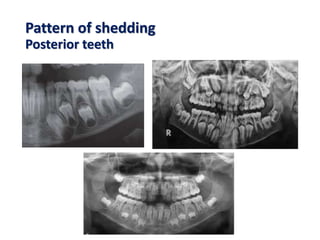
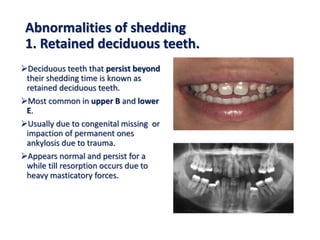
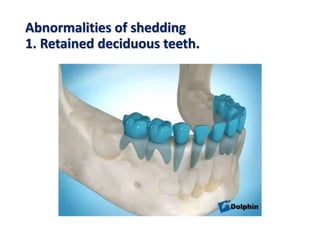
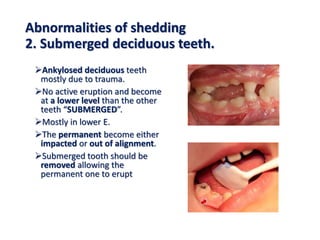
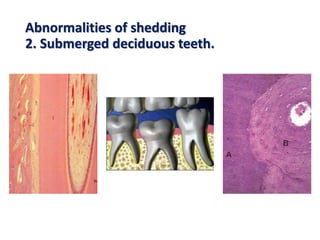
This document discusses tooth shedding, or the process by which primary teeth are replaced by permanent teeth. It defines shedding as the physiological process by which deciduous teeth are resorbed and lost to make way for successor teeth. Key points covered include the factors affecting shedding like pressure from erupting permanent teeth and genetic factors; the histology of shedding involving resorption of dental hard and soft tissues; the typical pattern of shedding from anterior to posterior teeth; and potential abnormalities in shedding like retained, submerged, or residual primary teeth.






































































![H.d. ii 11 [1]](https://cdn.slidesharecdn.com/ss_thumbnails/hsgwps6bsfel4qvanndn-signature-a5fad7992c1f4aa6df744a108dbfc10e79434281f3c12413d51643bf18458881-poli-171206182504-thumbnail.jpg?width=640&height=640&fit=bounds)



















