Downloaded 322 times

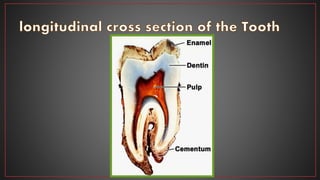
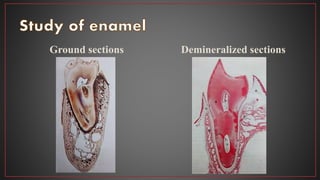
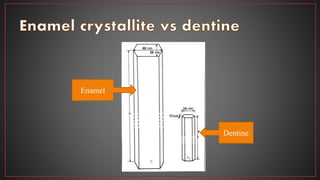
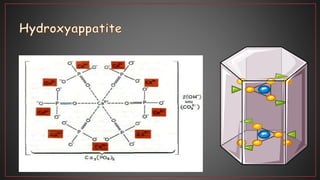
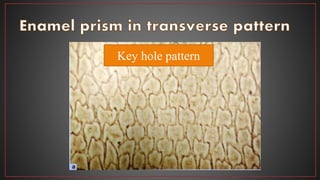
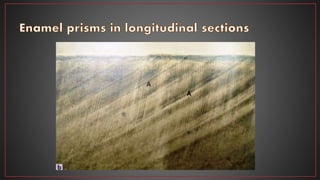
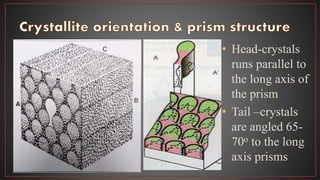
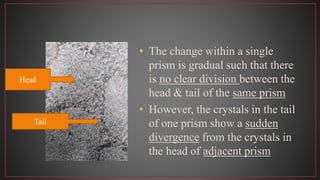
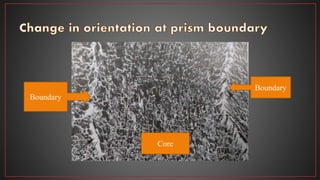
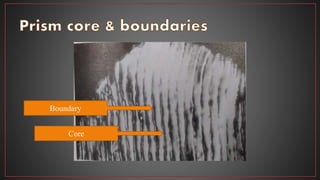

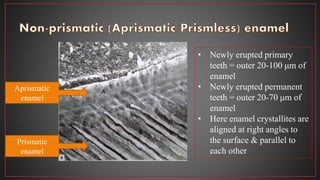
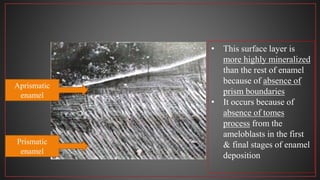


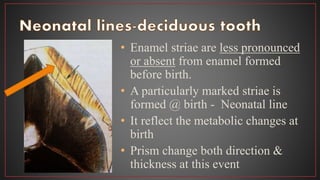
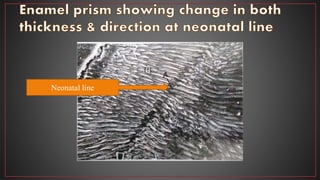
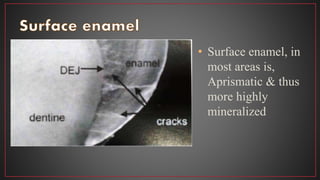
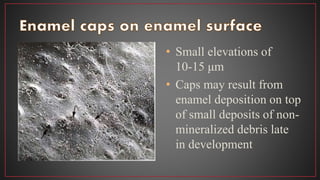








This document provides details on the structure and composition of enamel. It notes that enamel is the hardest tissue in the body, covering the anatomical crown. It is made up primarily of hydroxyapatite crystals arranged in enamel prisms/rods from the dentin-enamel junction to the surface. The direction of the prisms changes in a sinusoidal pattern. Between the prisms is interprismatic enamel. Near the surface is aprismatic enamel which is more highly mineralized. Throughout life, the crown is covered by an organic layer or integument.



































































