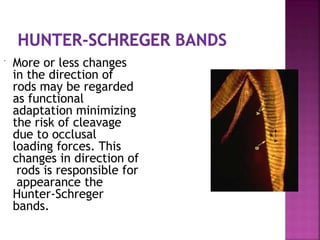
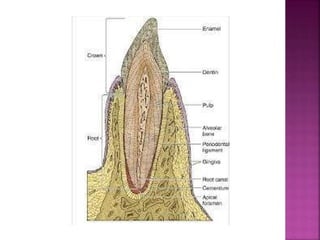
Enamel is the hardest tissue in the human body, covering the anatomic crown of a tooth, primarily consisting of acellular, highly mineralized hydroxyapatite crystals. It protects the underlying dentin, has varying thickness, and its physical properties include high hardness, brittleness, and specific solubility characteristics. The development and structure of enamel involve intricate biological processes, including the role of ameloblasts, leading to potential structural defects such as hypoplasia and discoloration from various factors.

![ Calcium
hydroxyapatite
[Ca10(PO4)6(OH)2].
The mineral content
increases from the DEJ
to the surface.
Most crystallites are
regularly hexagonal in
cross-section.](https://image.slidesharecdn.com/enamel-1-241104173841-cc3ad0e0/85/enamel-strogest-teeth-structure-on-the-body-13-320.jpg)