Download as PDF, PPTX






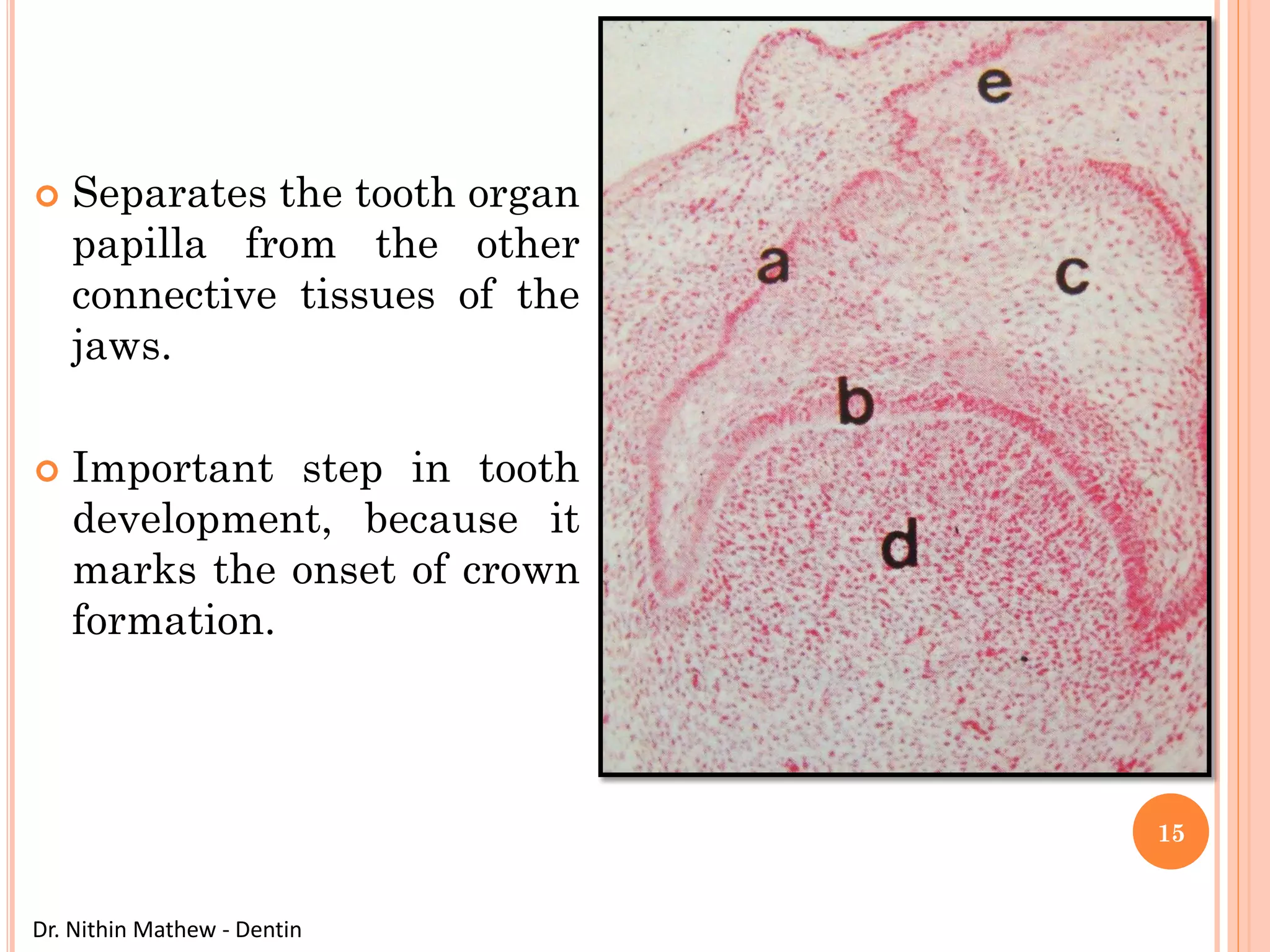
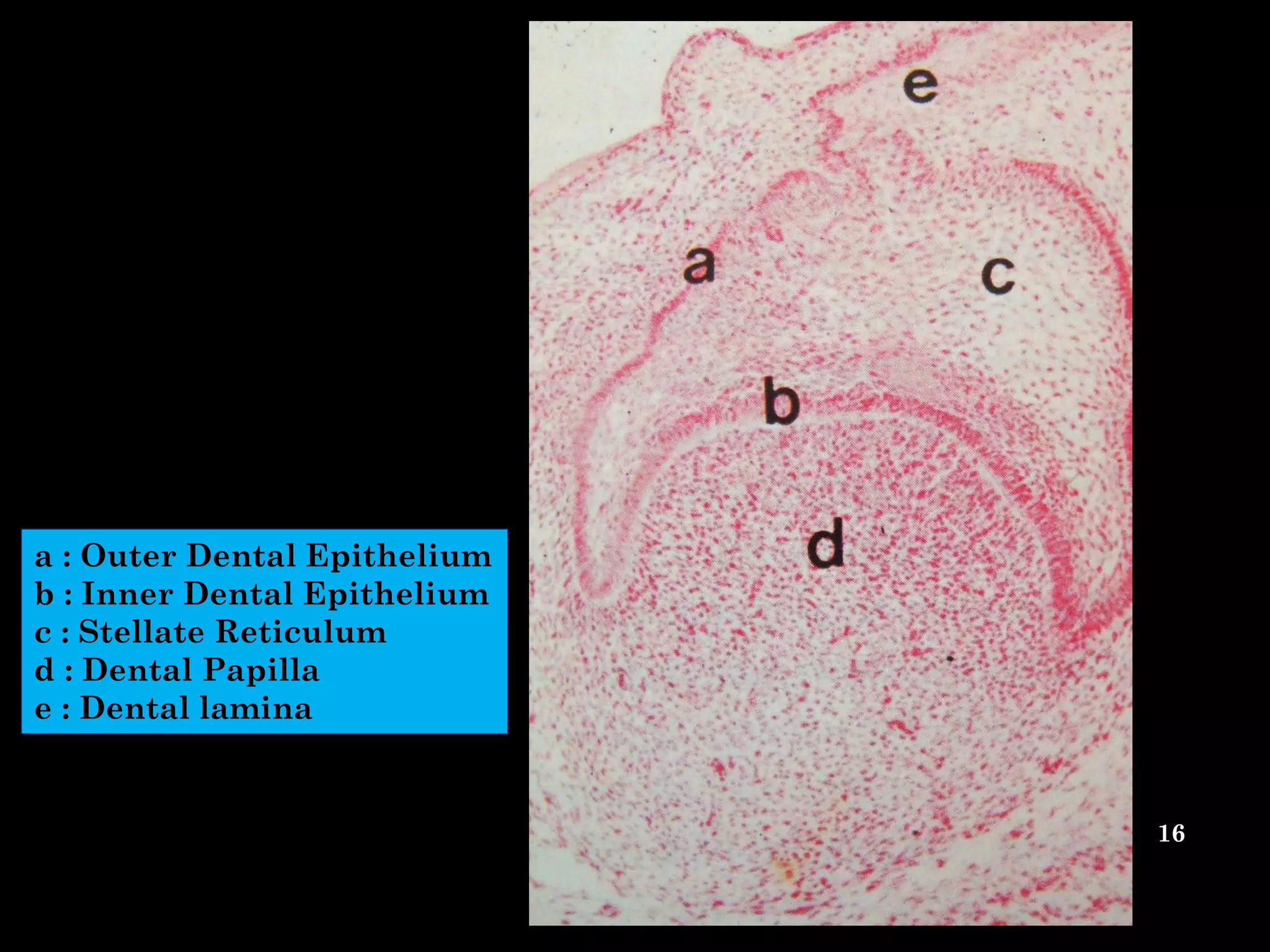


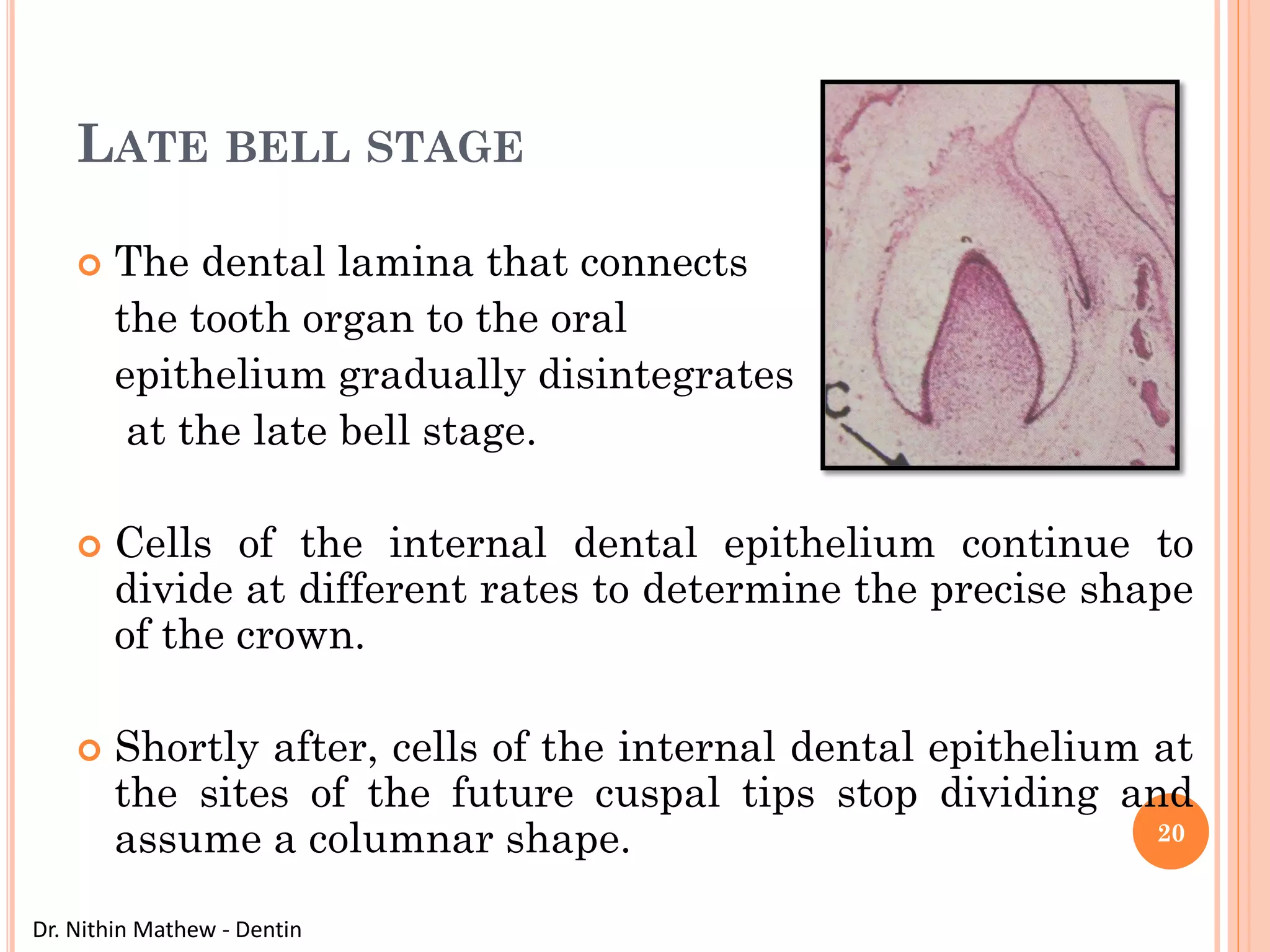
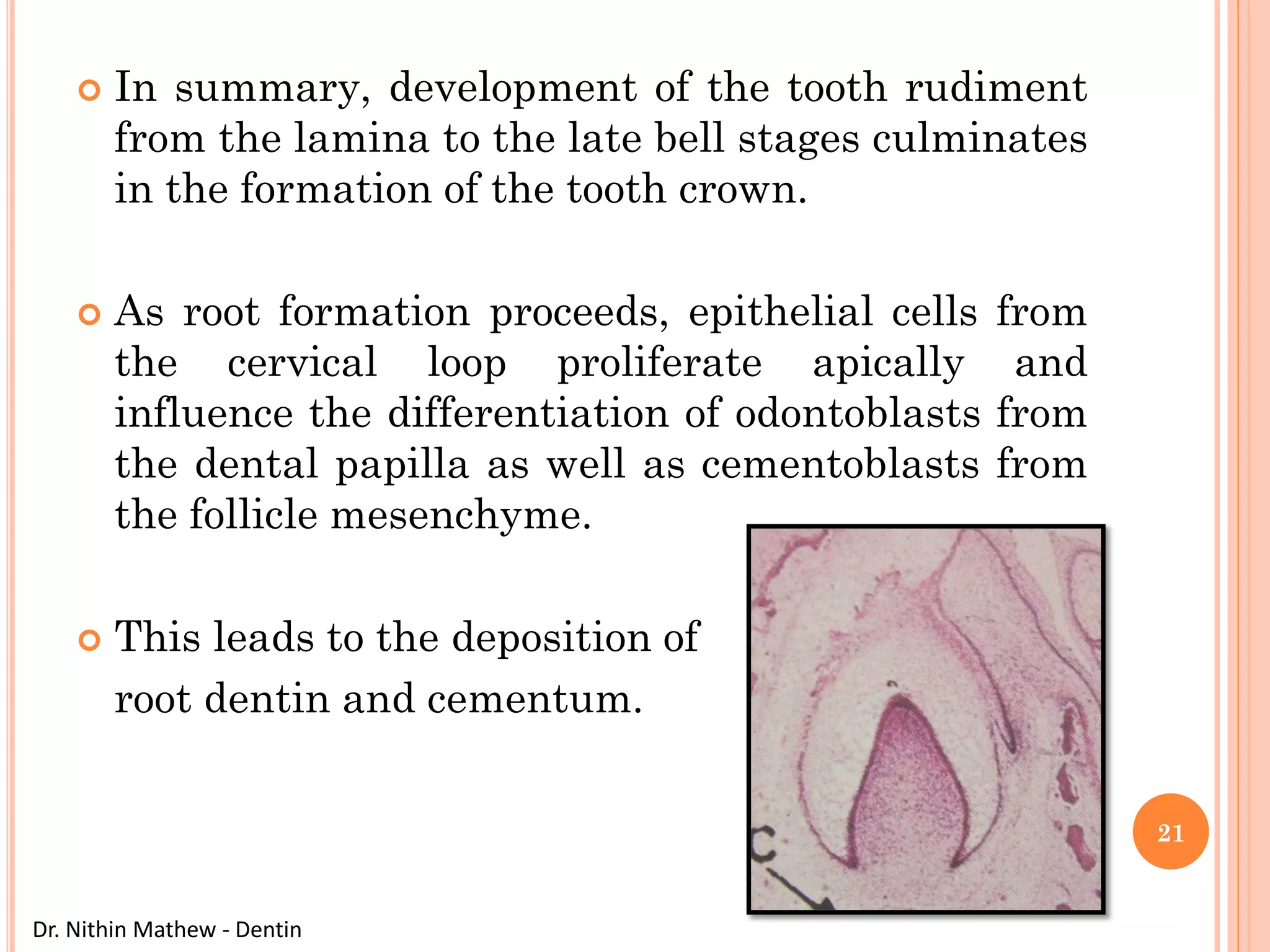
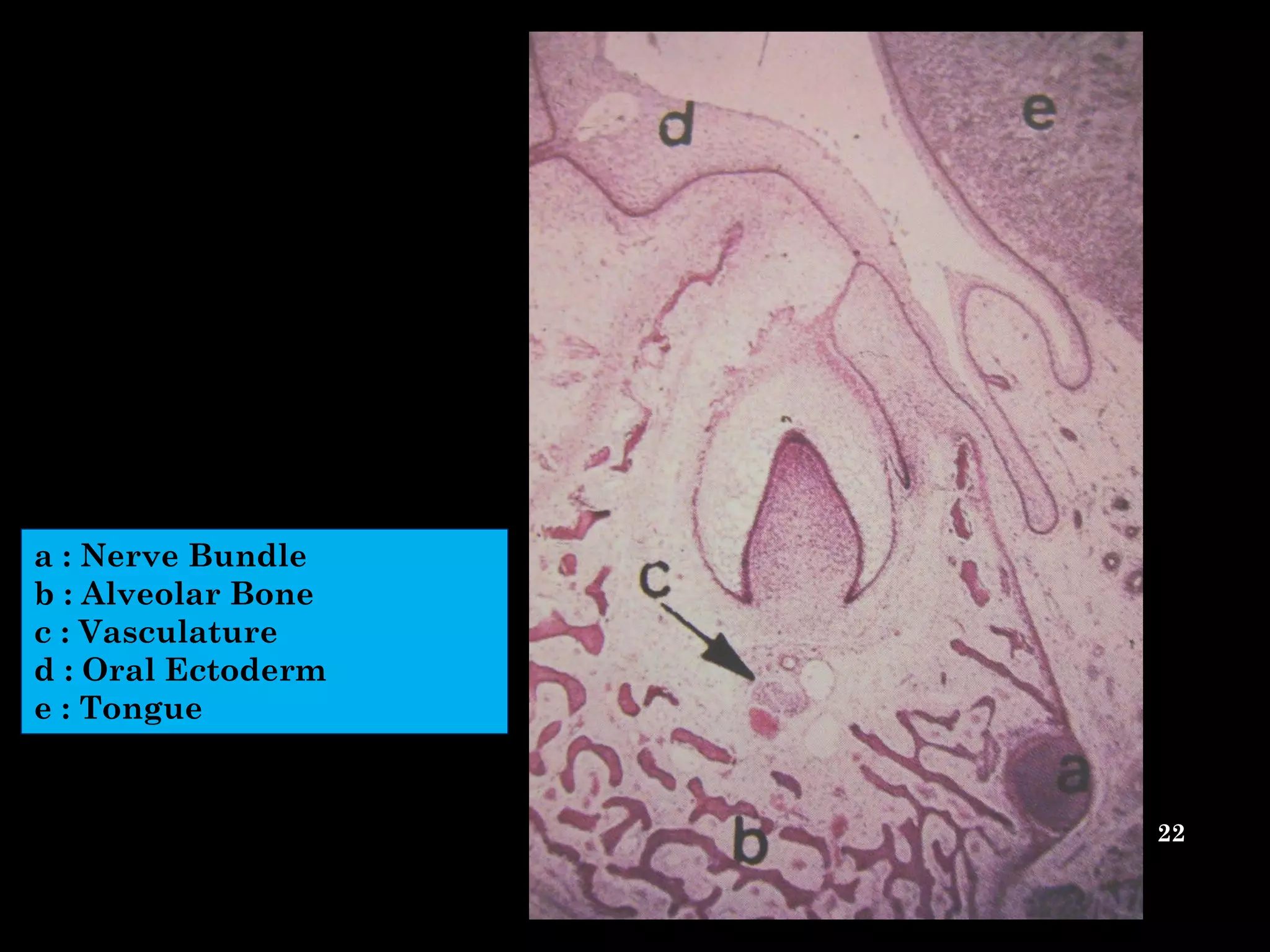
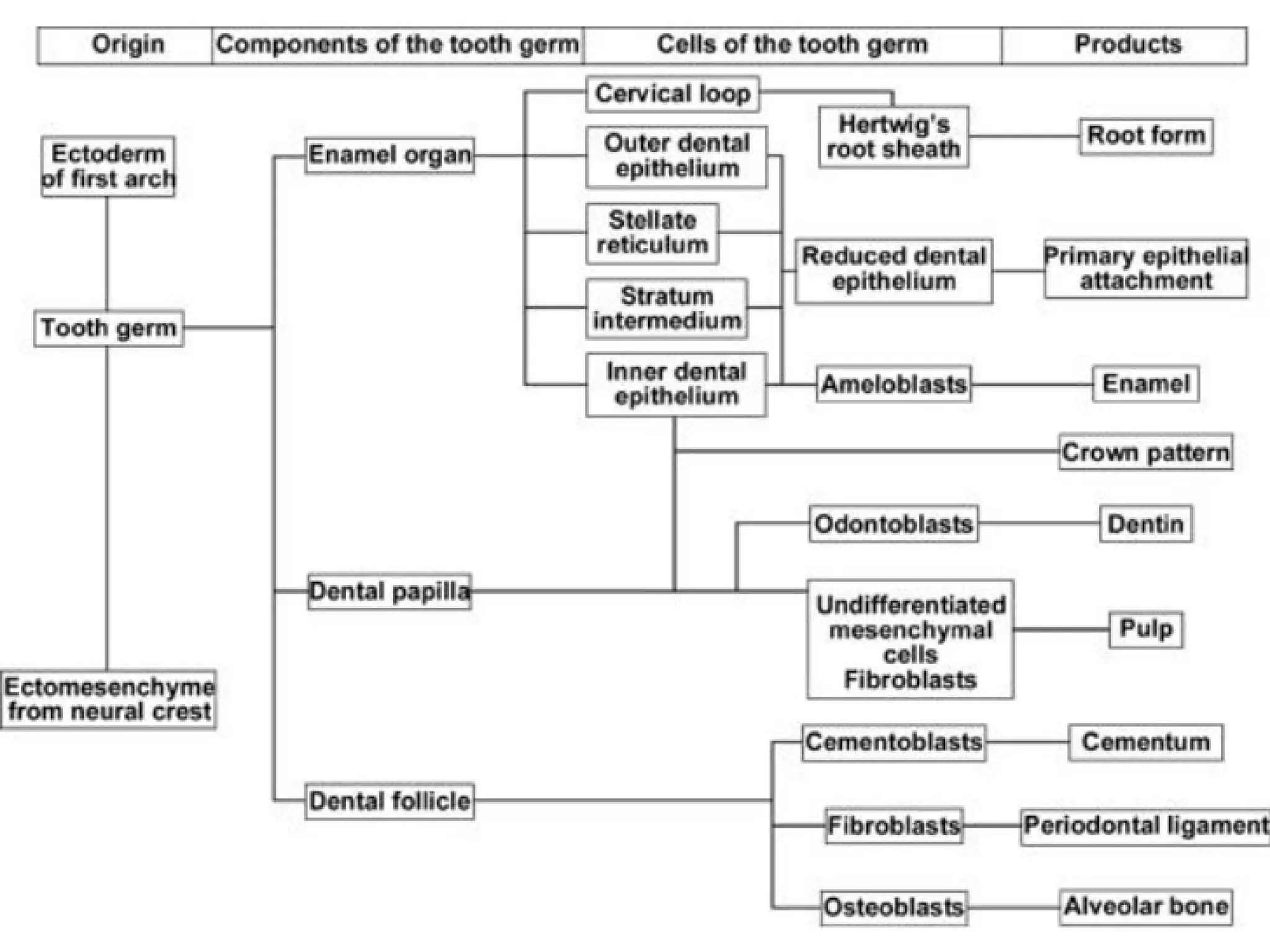
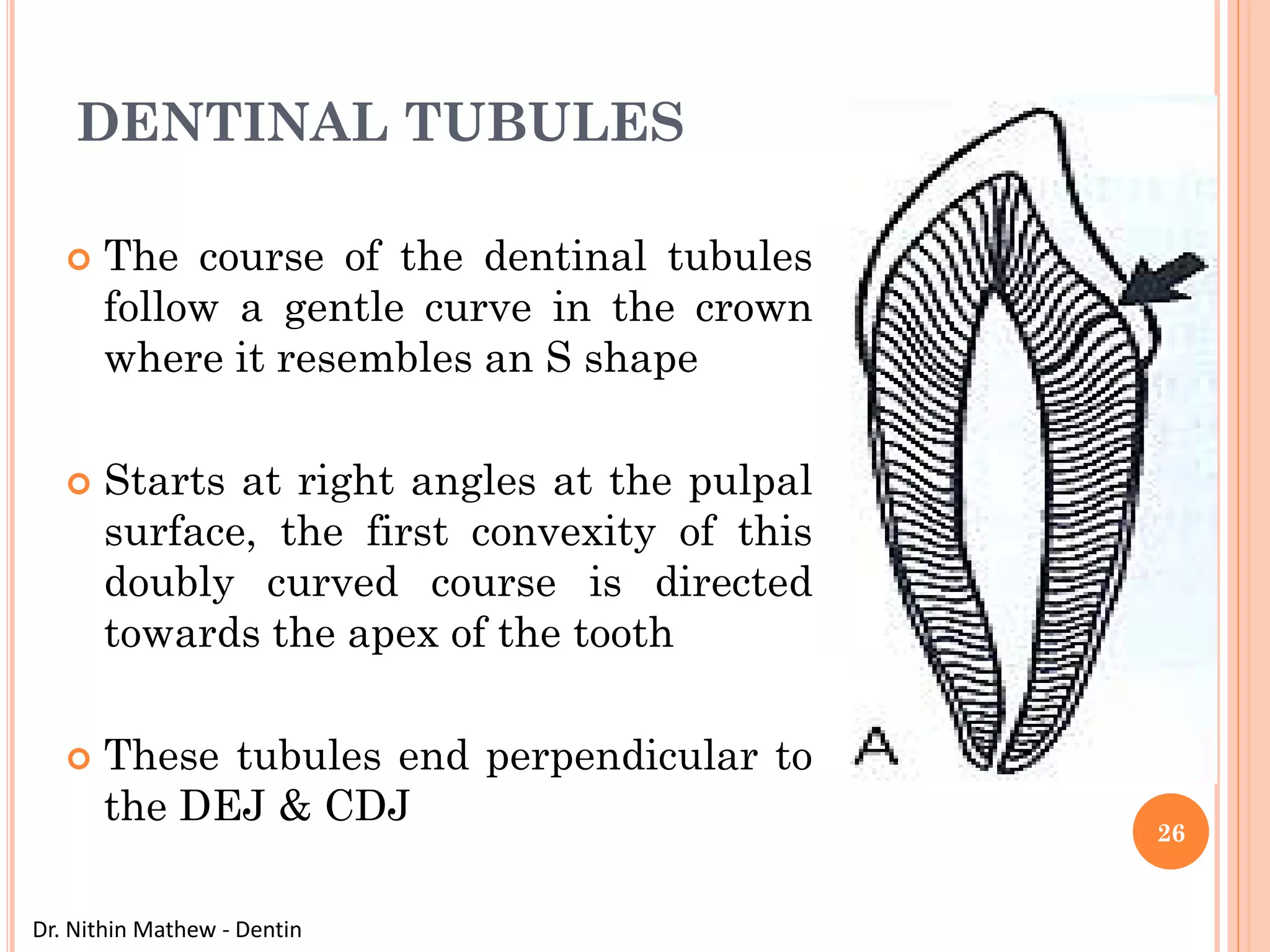
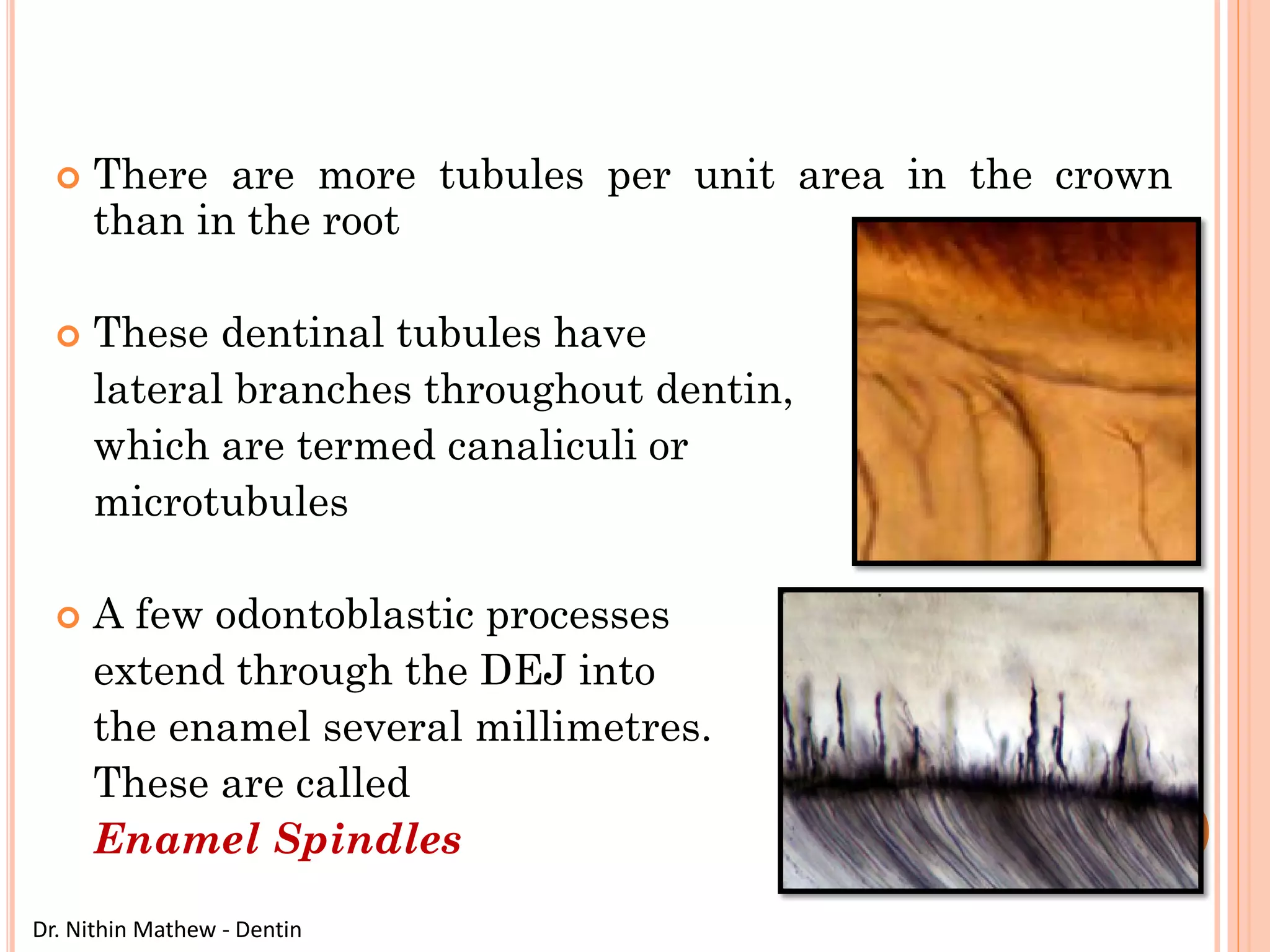
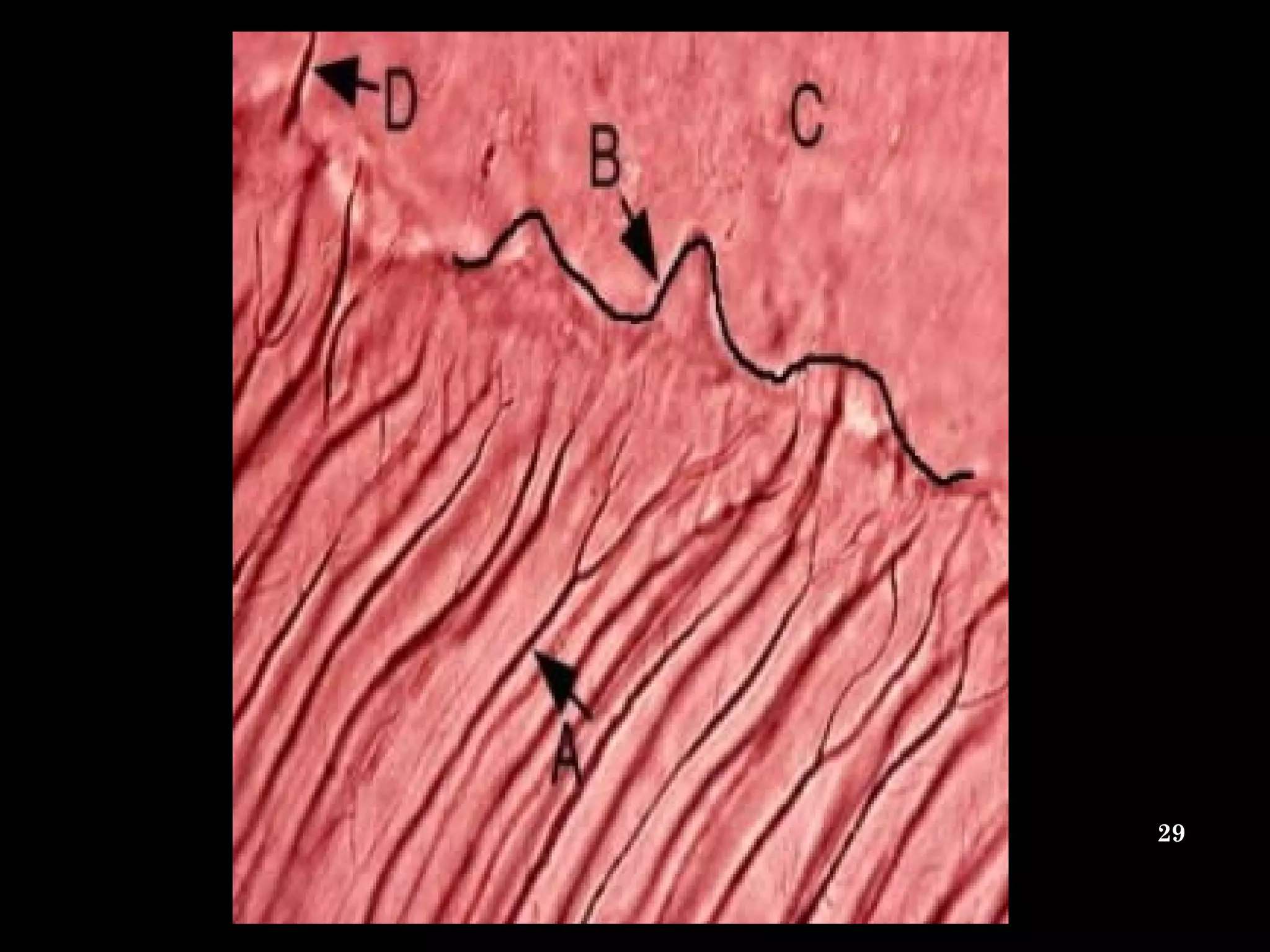
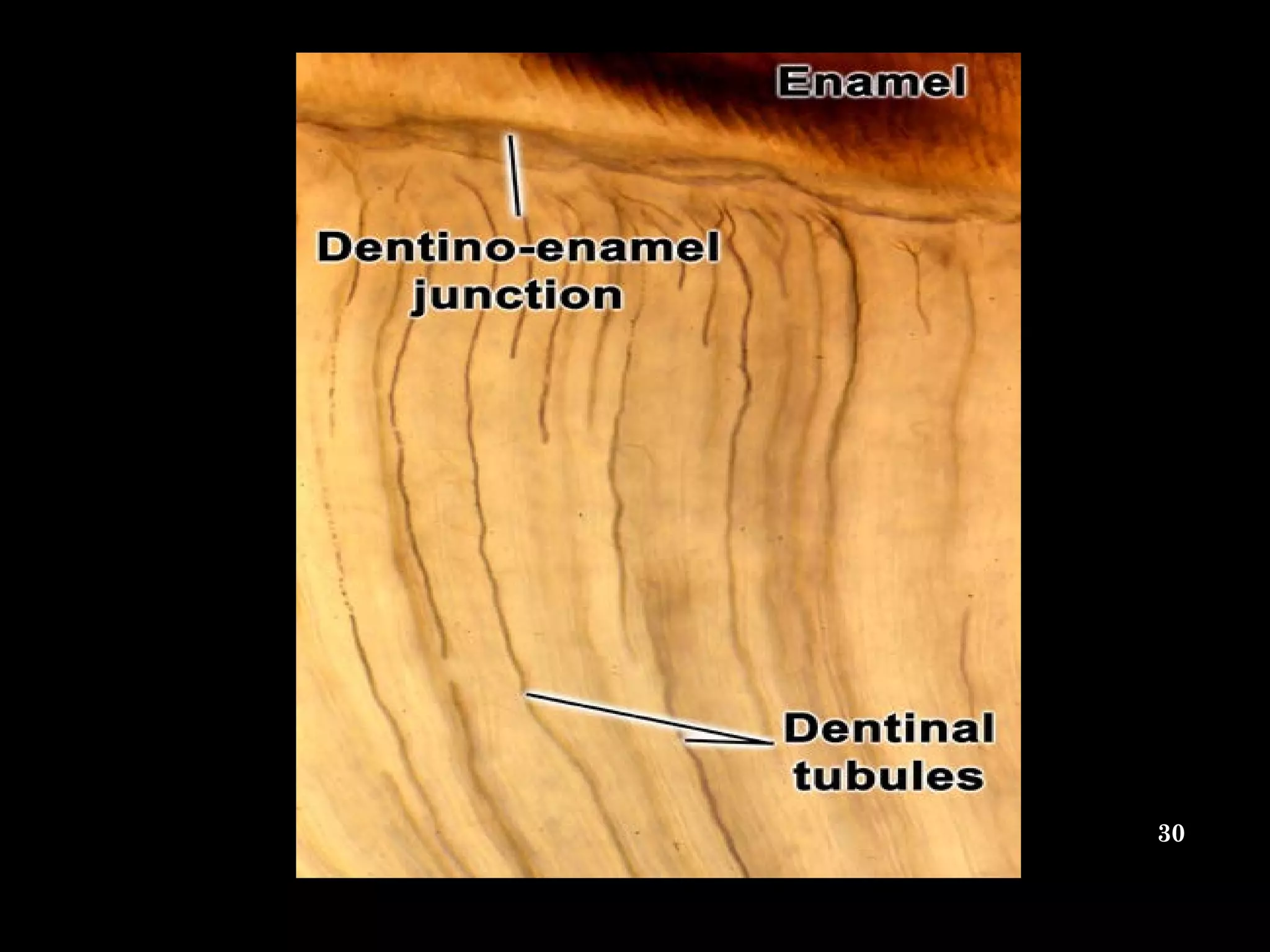

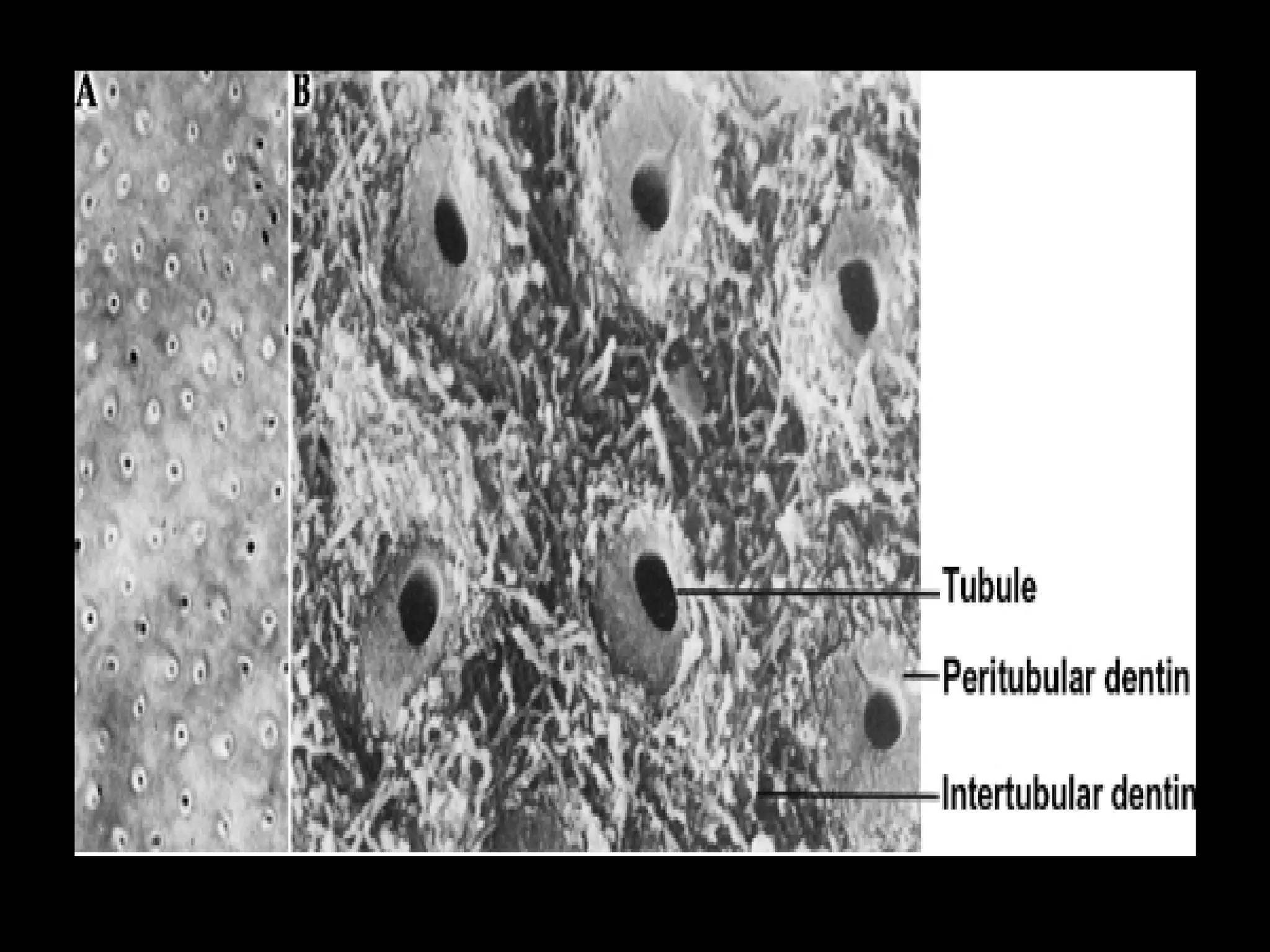
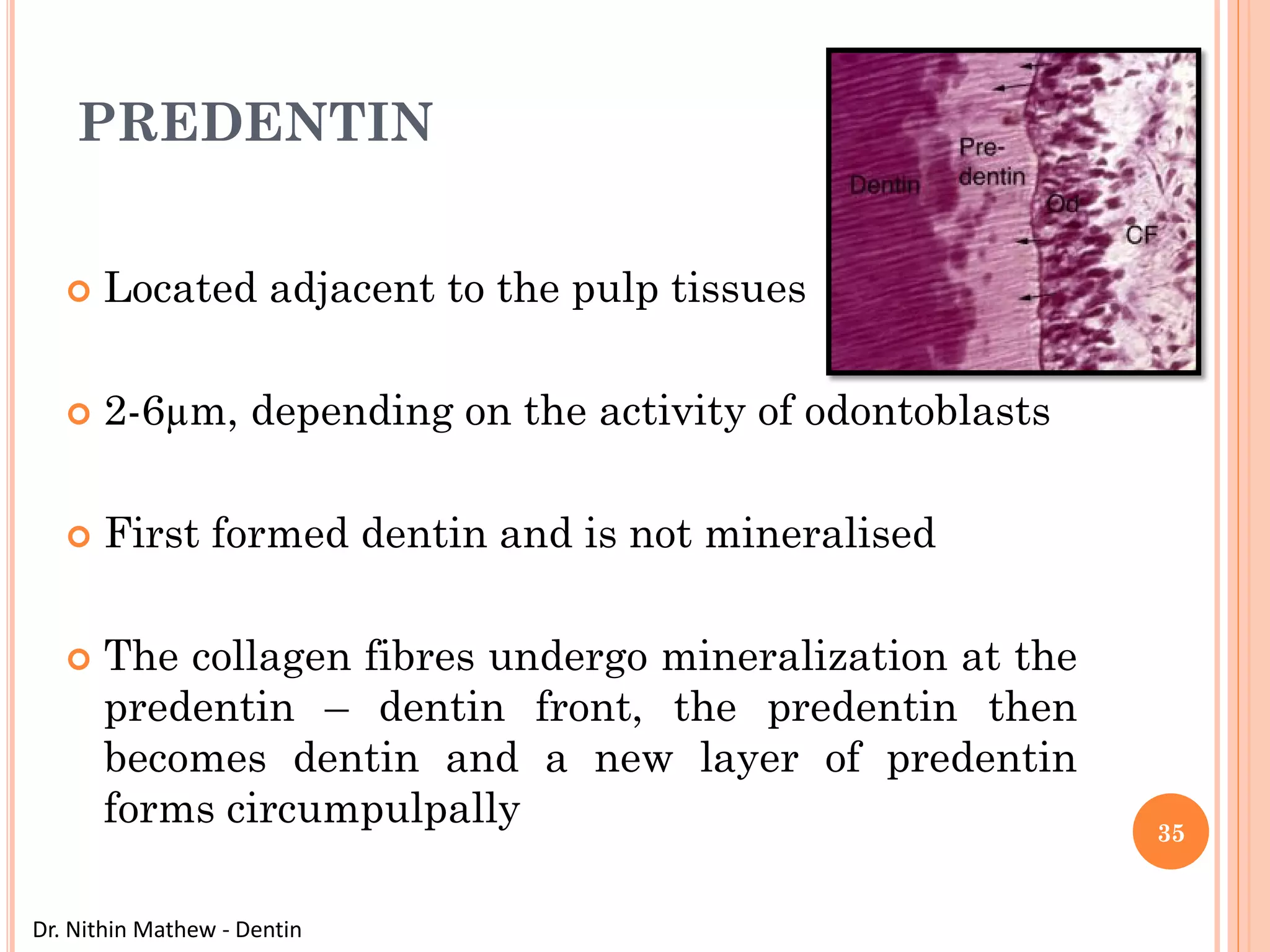
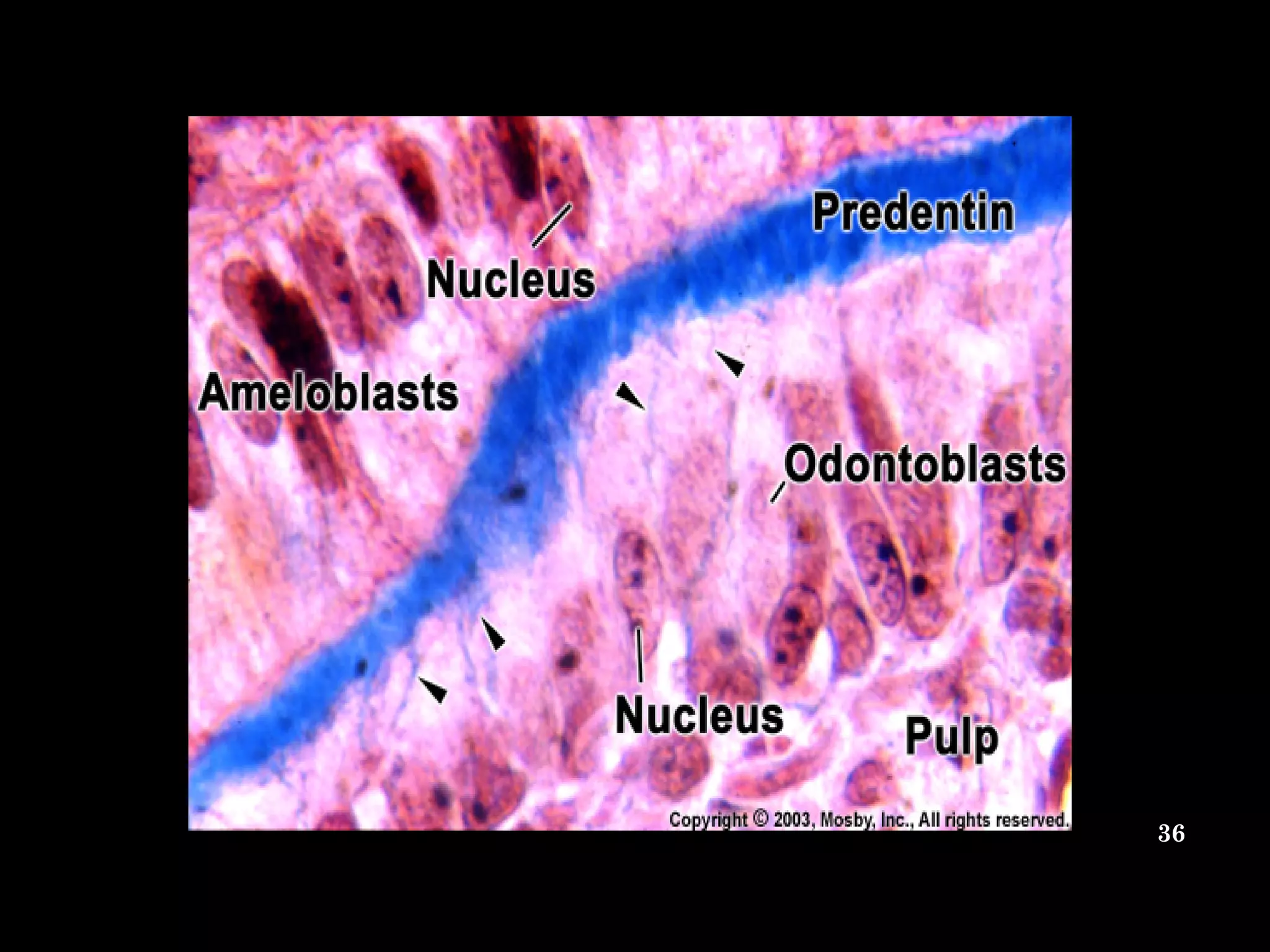
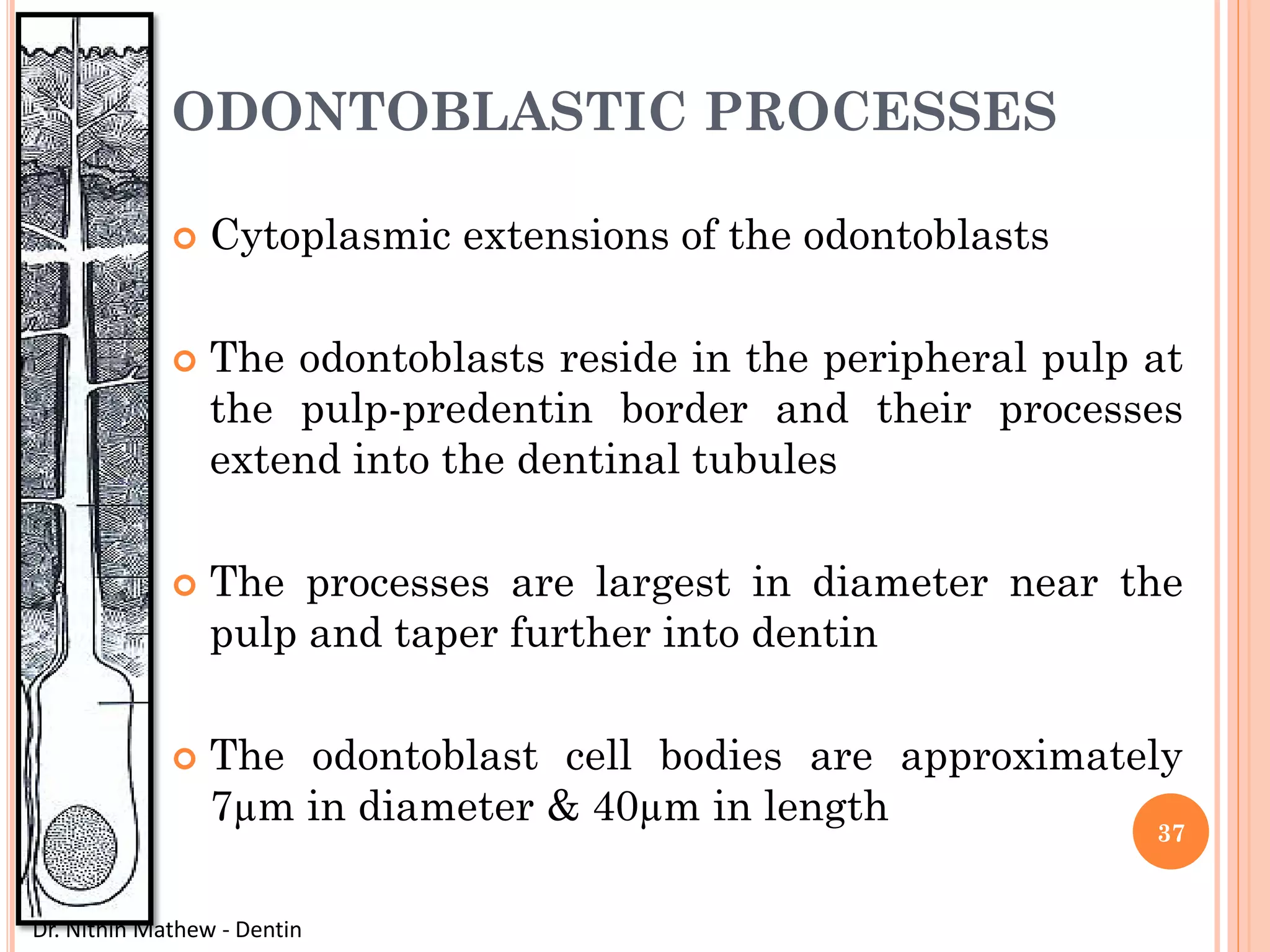
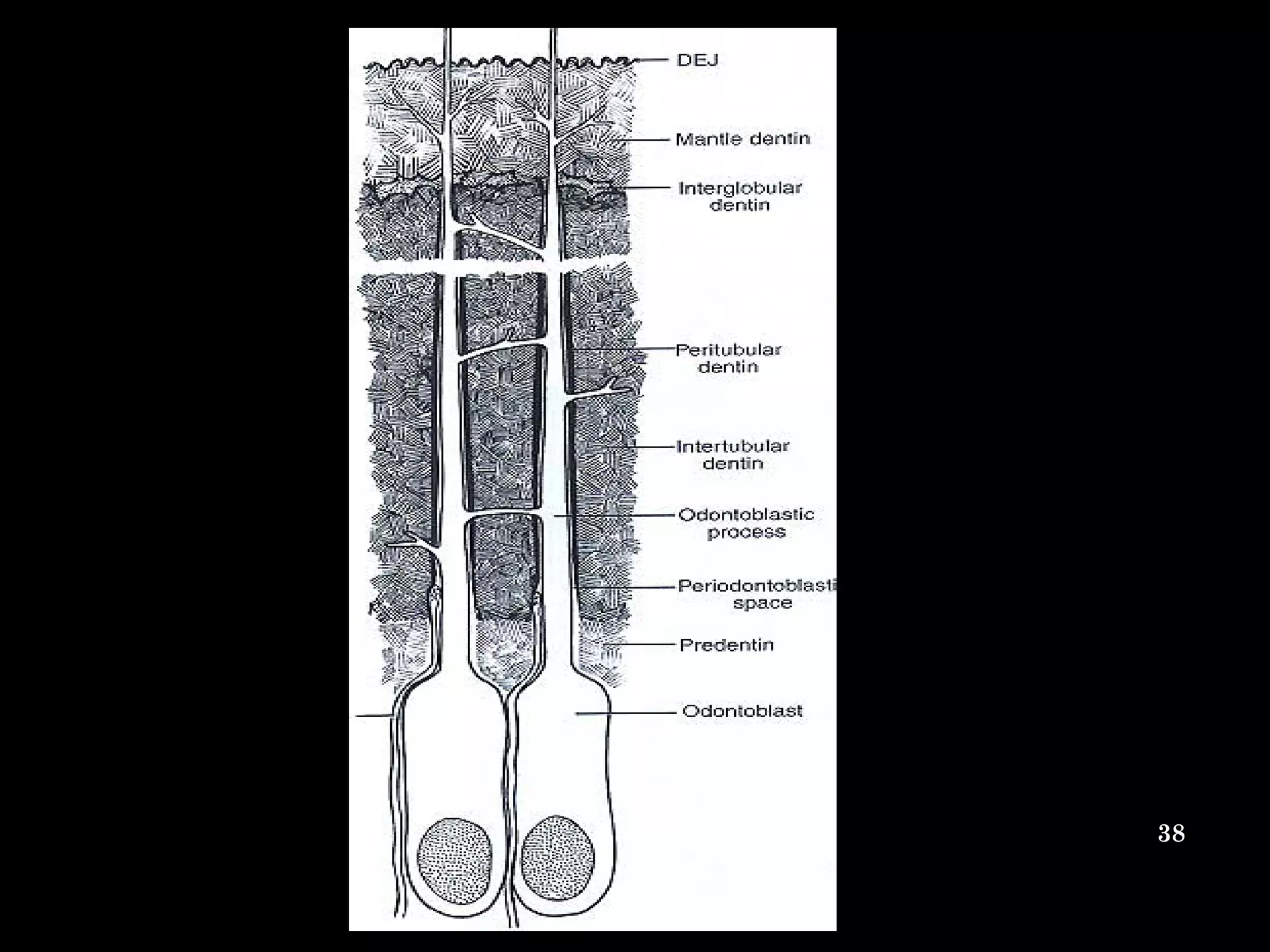


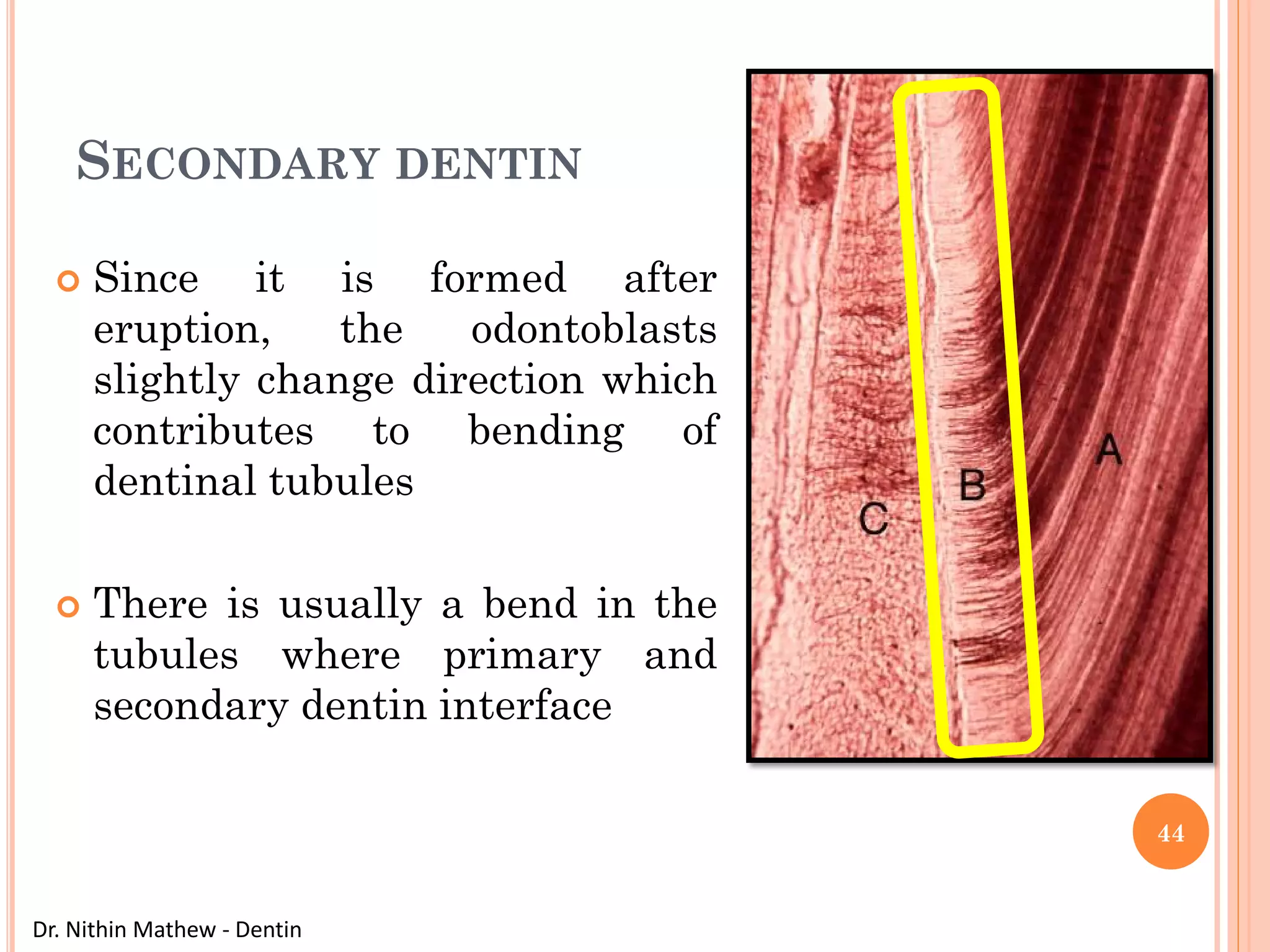
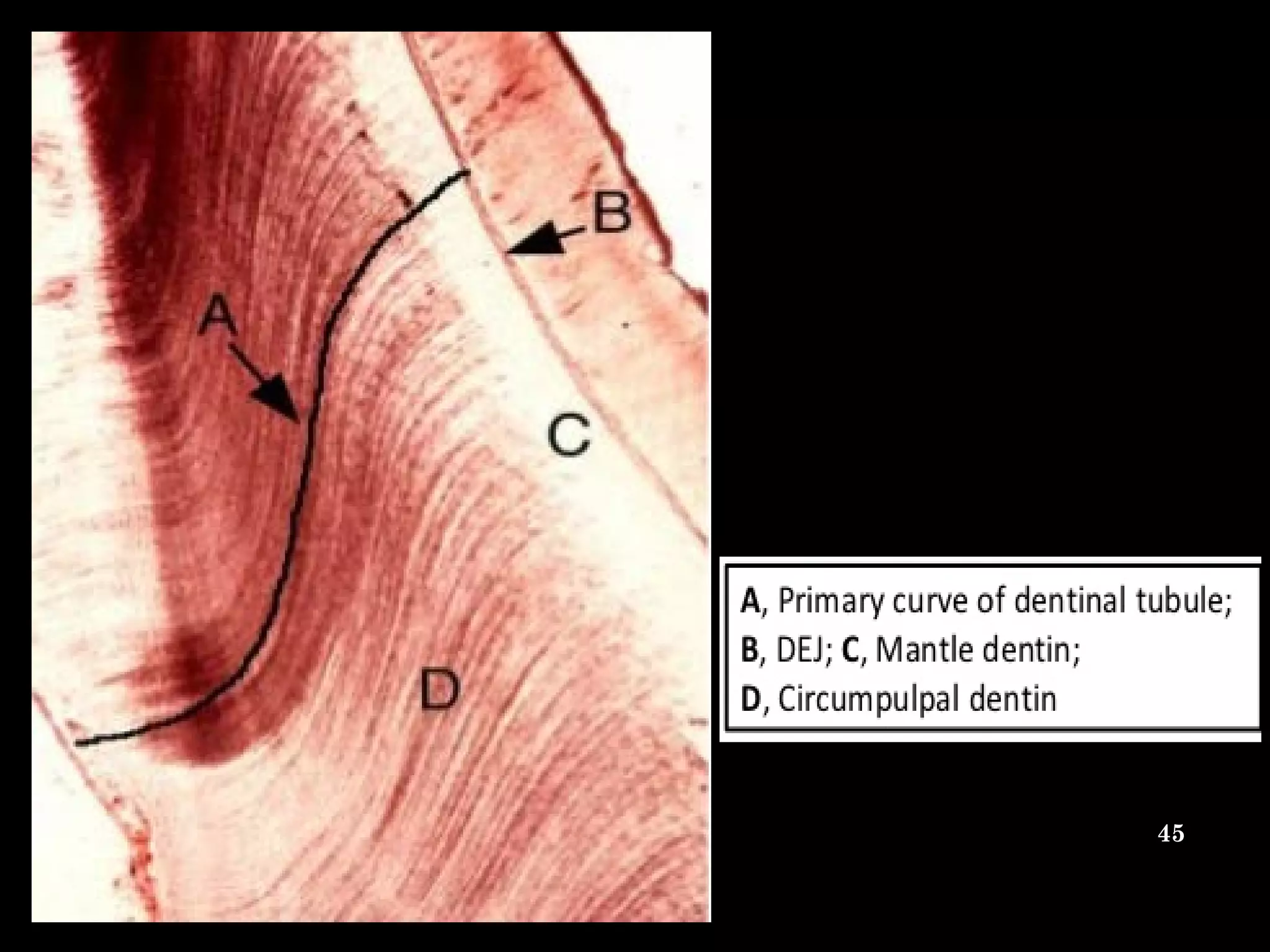
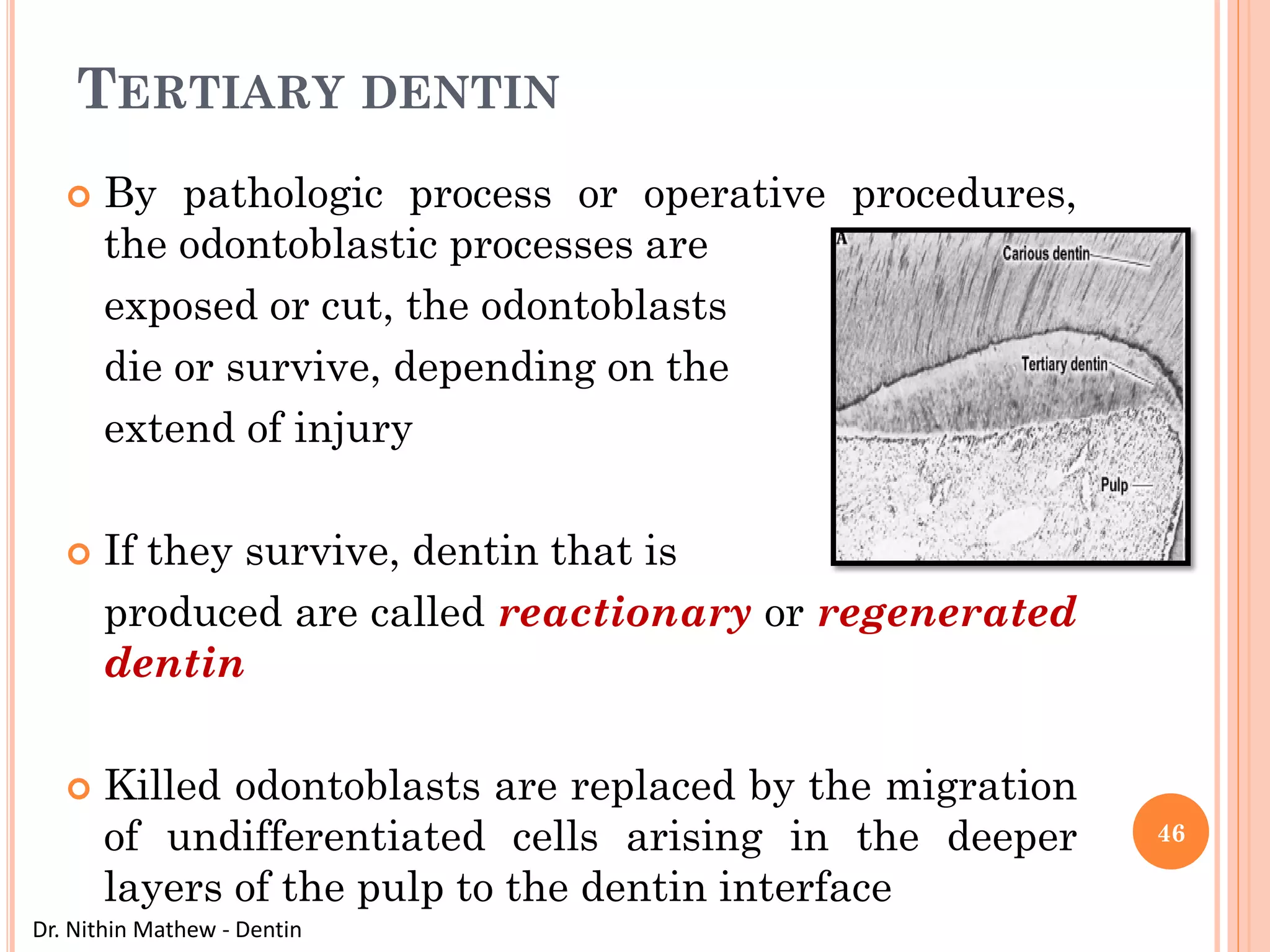

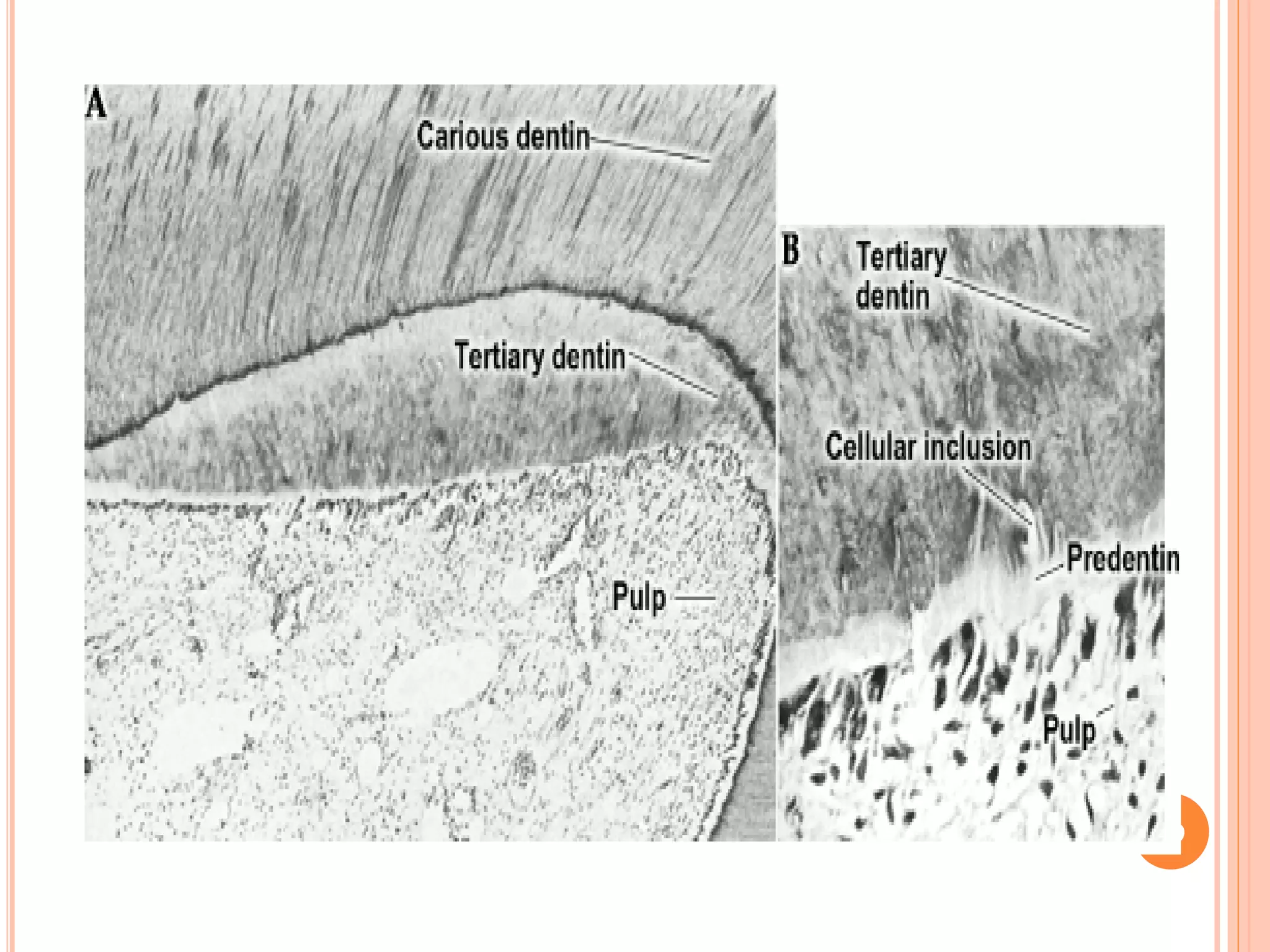





























The document discusses the structure and development of dentin. It describes dentin as the layer beneath enamel that provides shape and structure to teeth. Dentin forms in stages that mirror tooth development from the lamina bud stage through late bell stage. Key features of dentin include dentinal tubules that contain odontoblastic processes and layers like peritubular dentin, intertubular dentin, and predentin near the pulp. Dentin is laid down in primary, secondary, and tertiary forms throughout life.


































































































