Download as PDF, PPTX


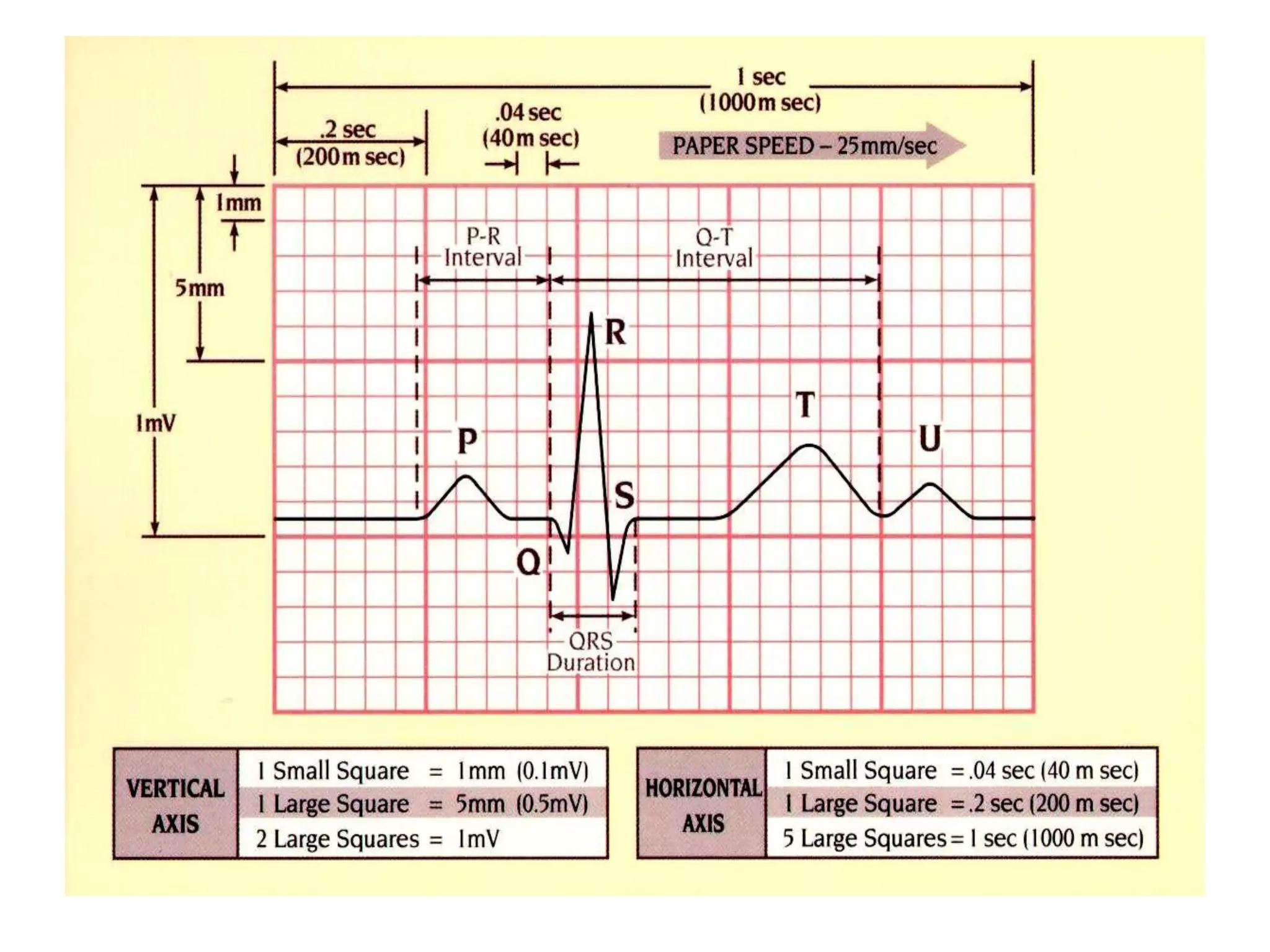







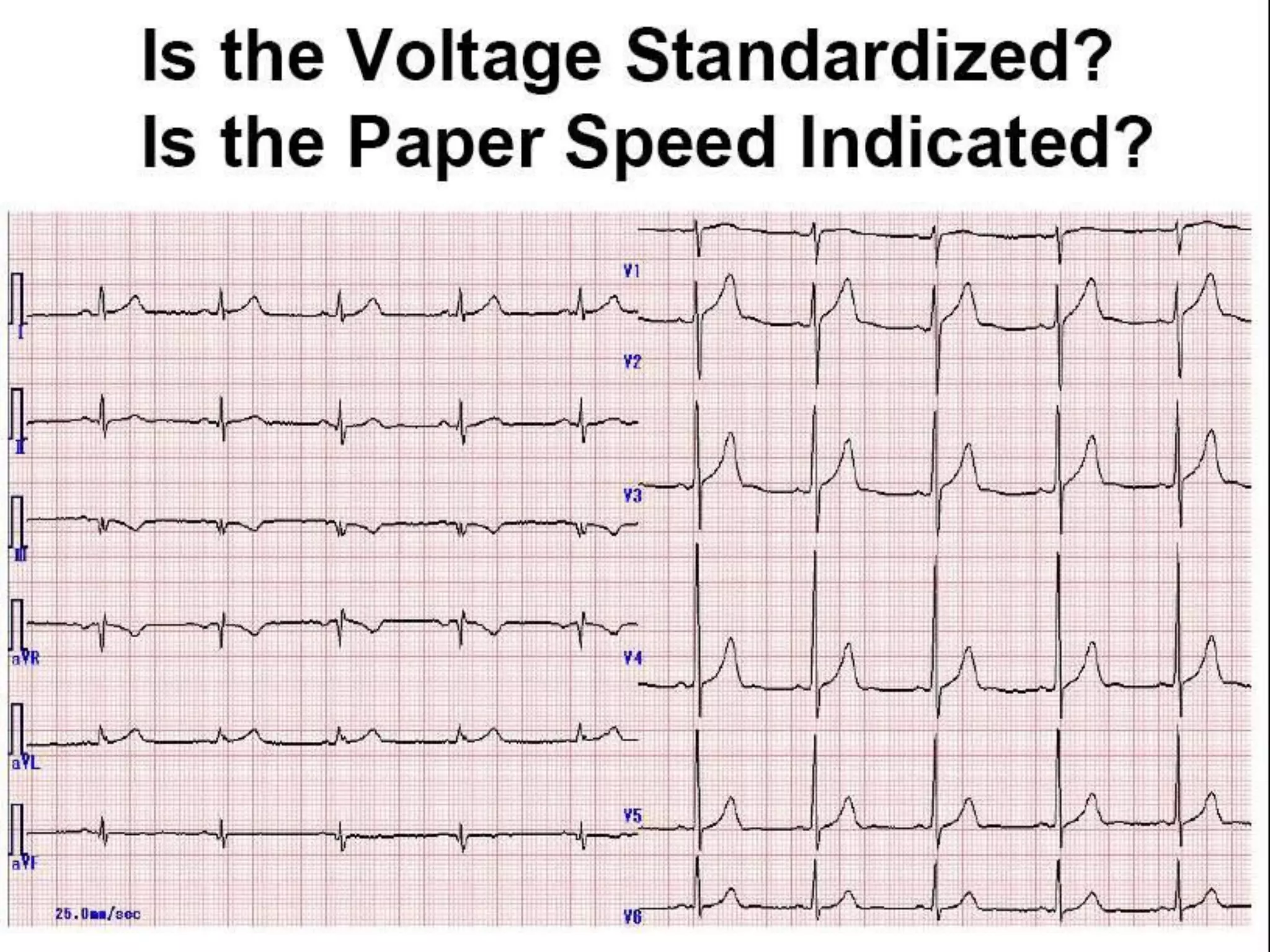














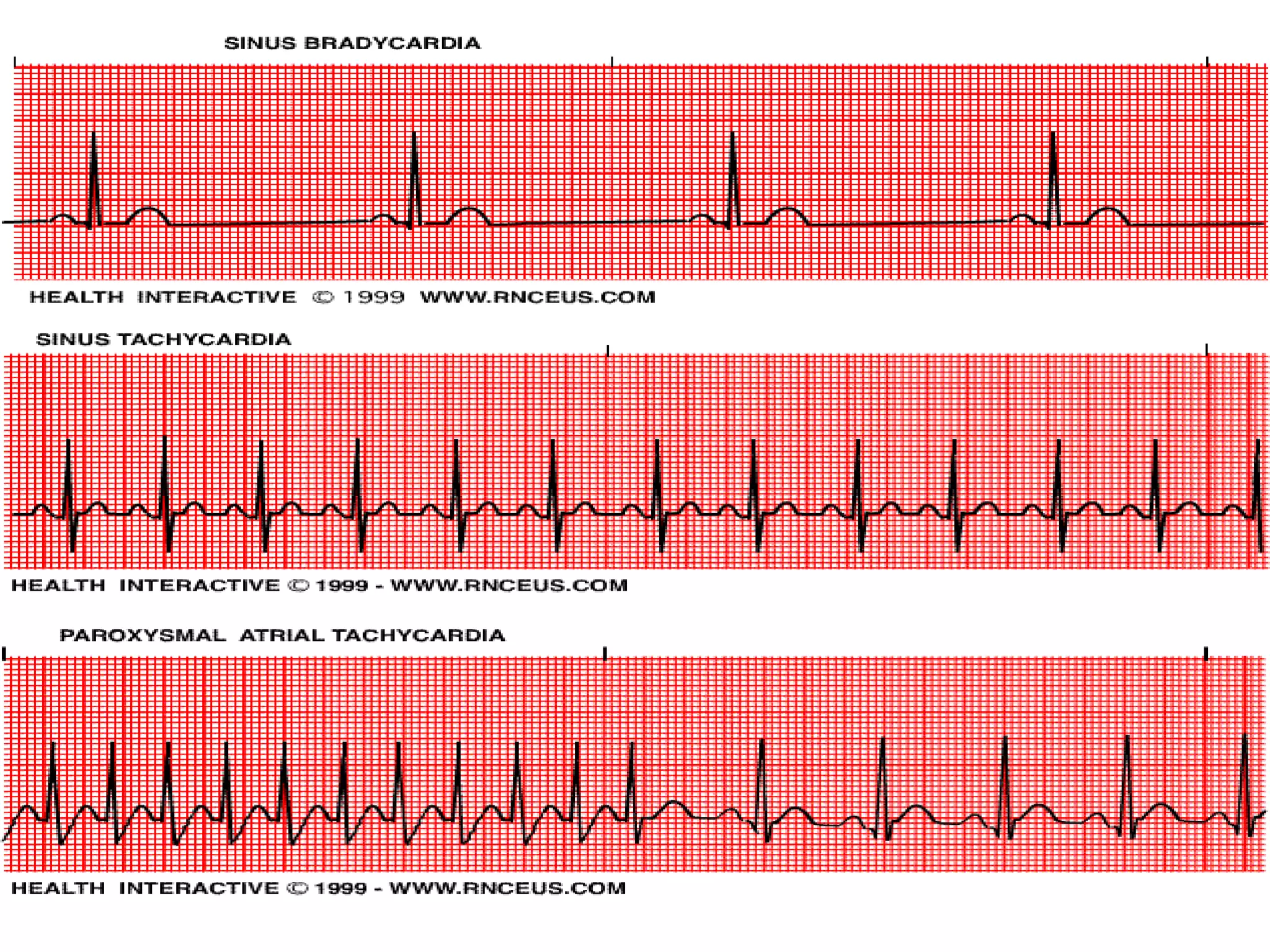
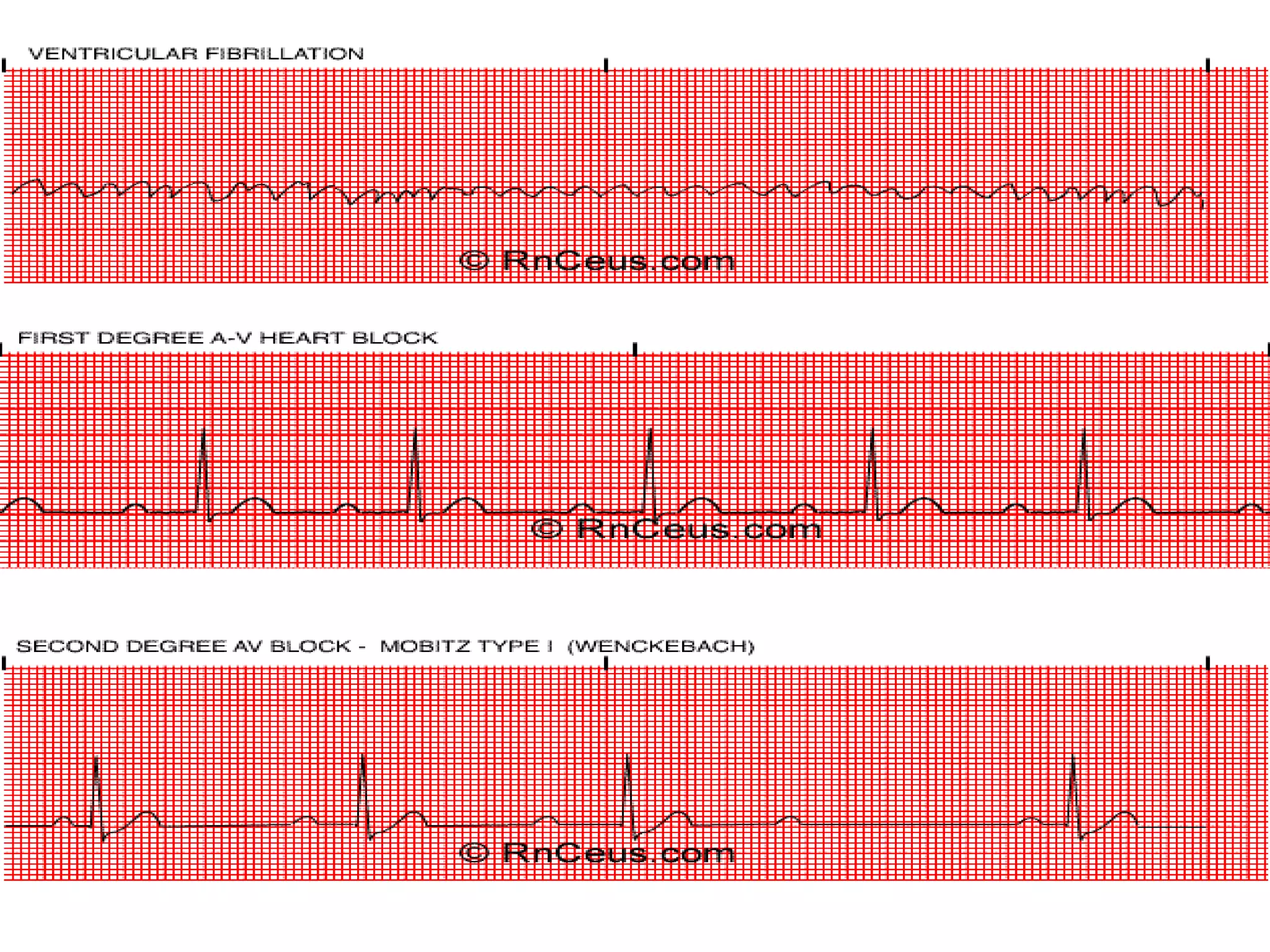


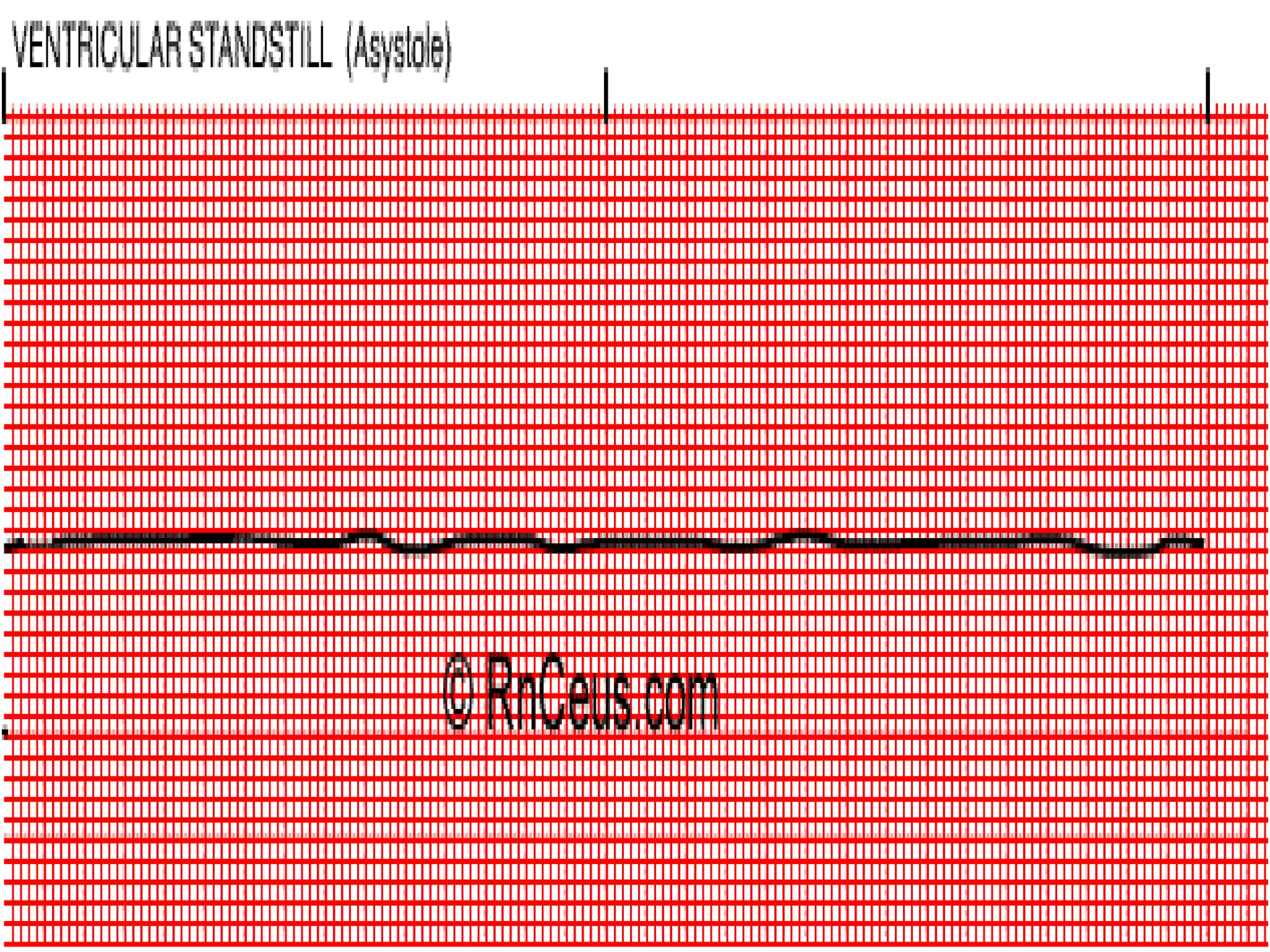






































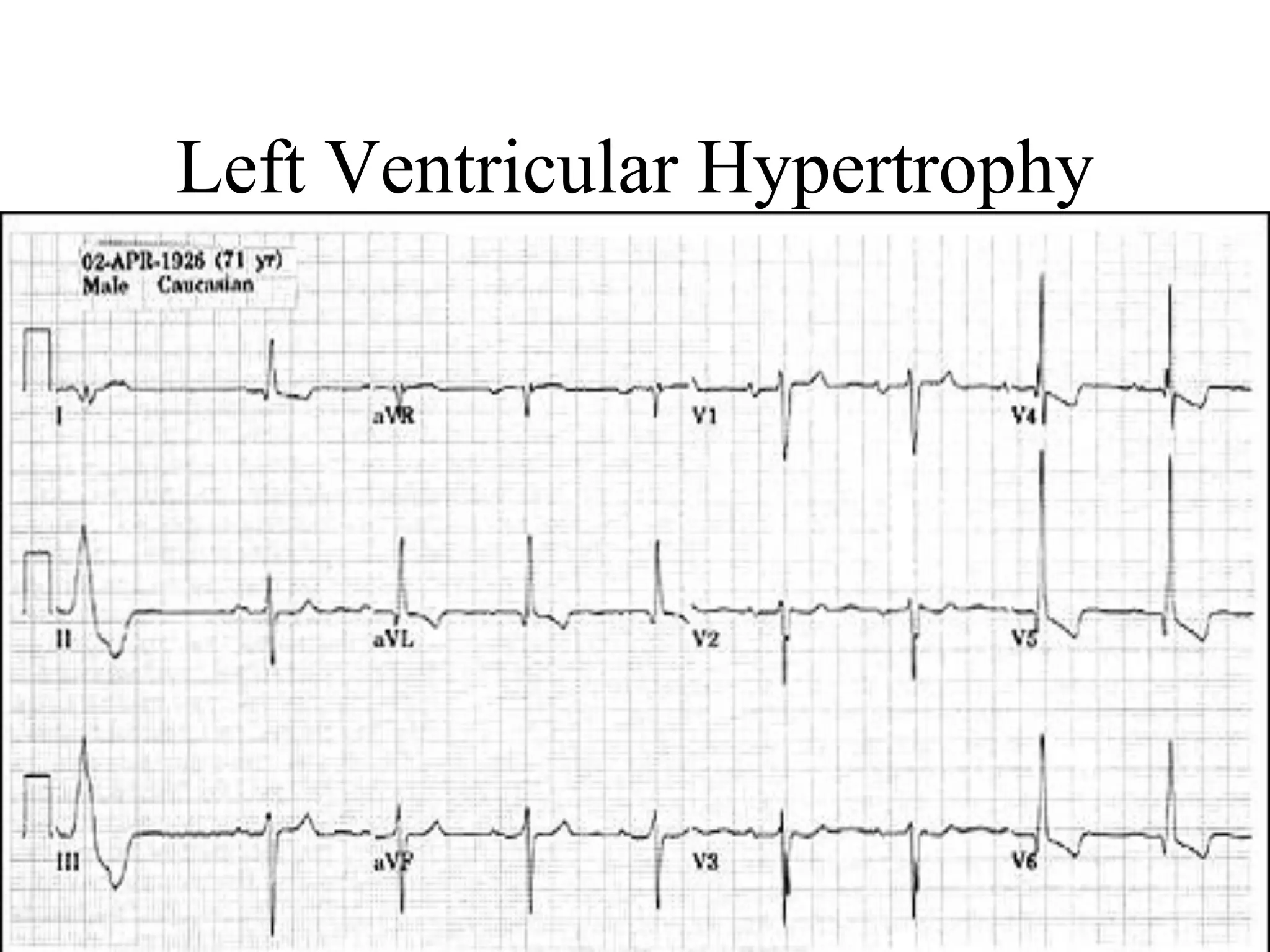
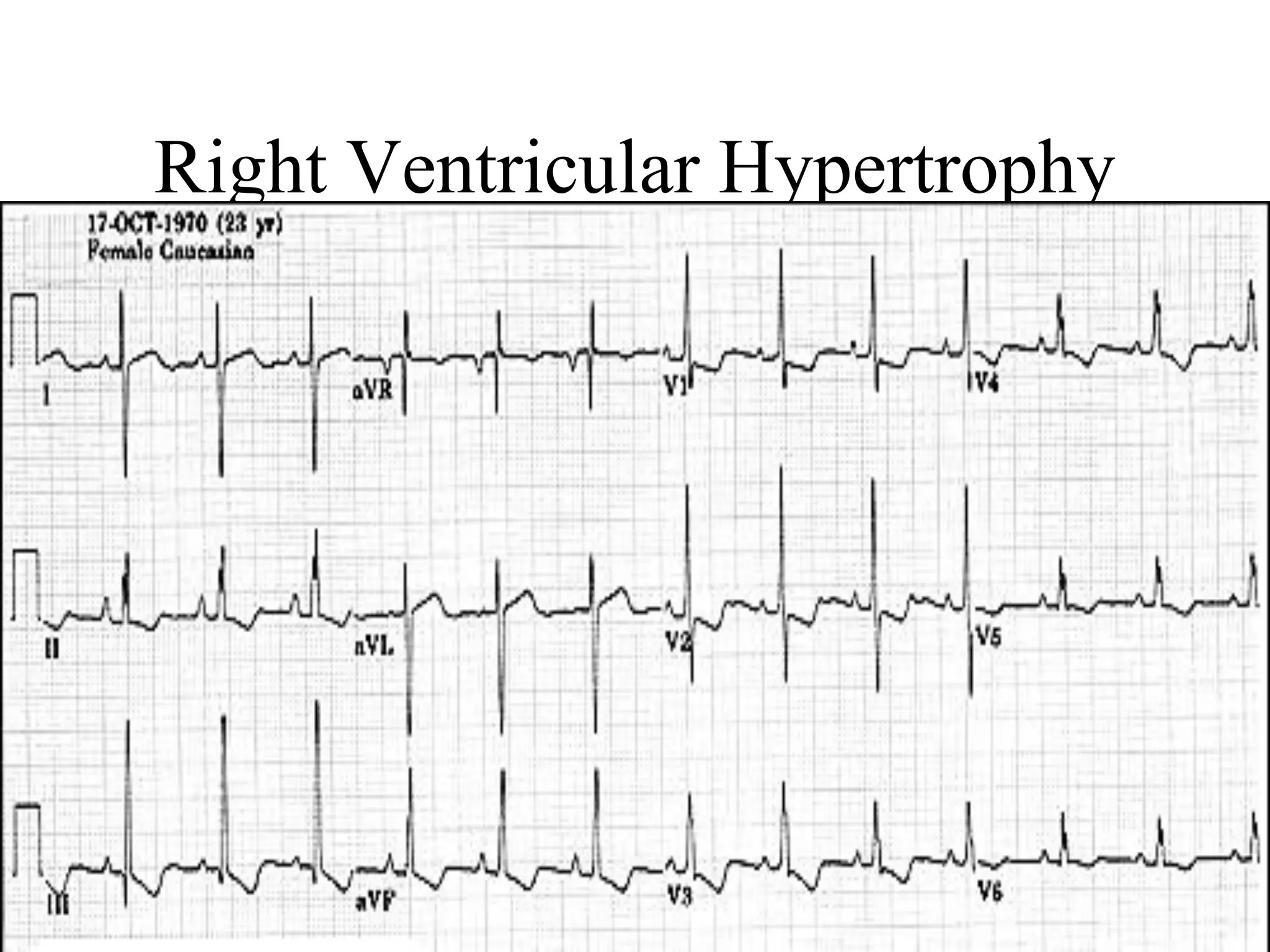















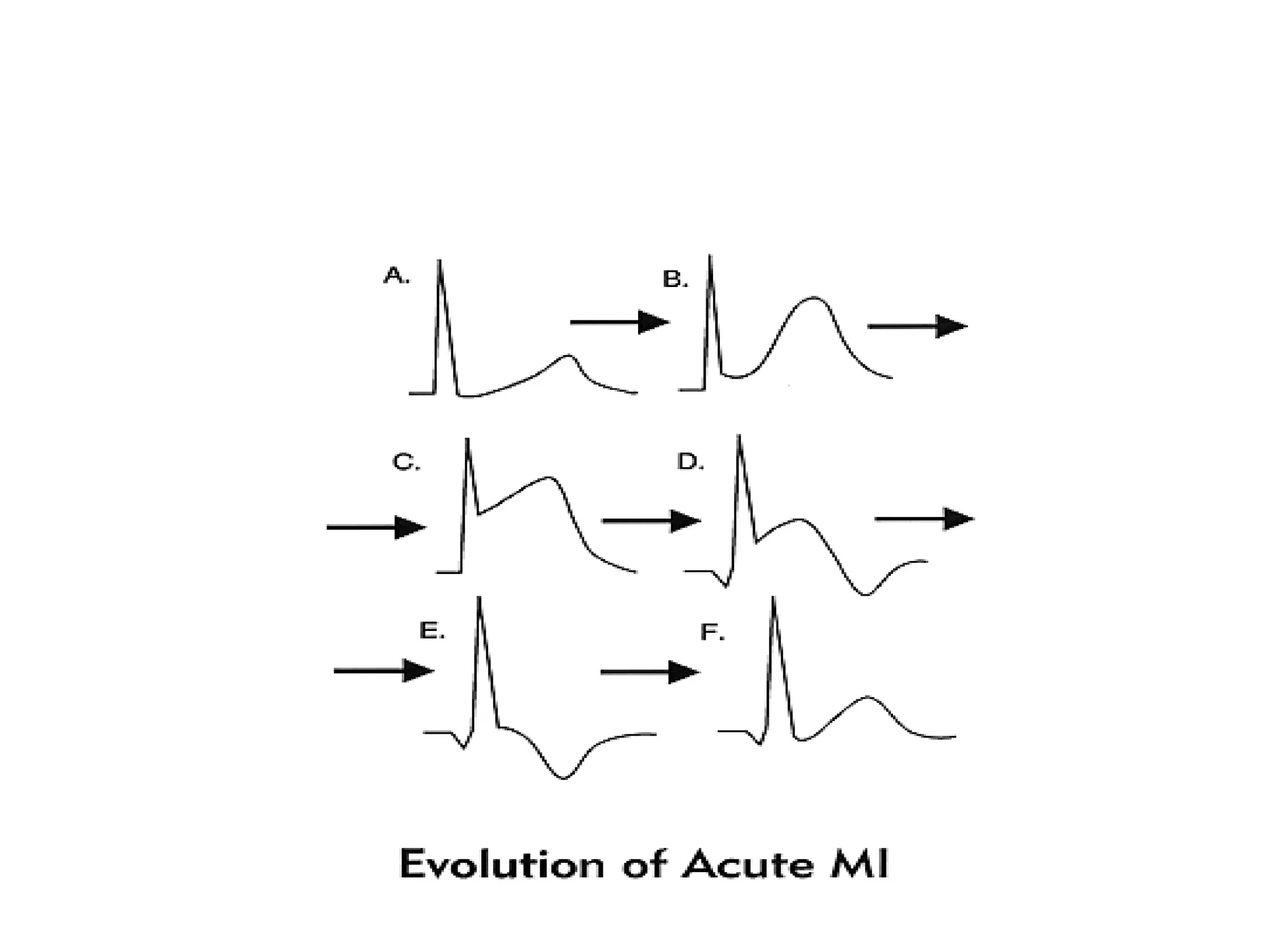





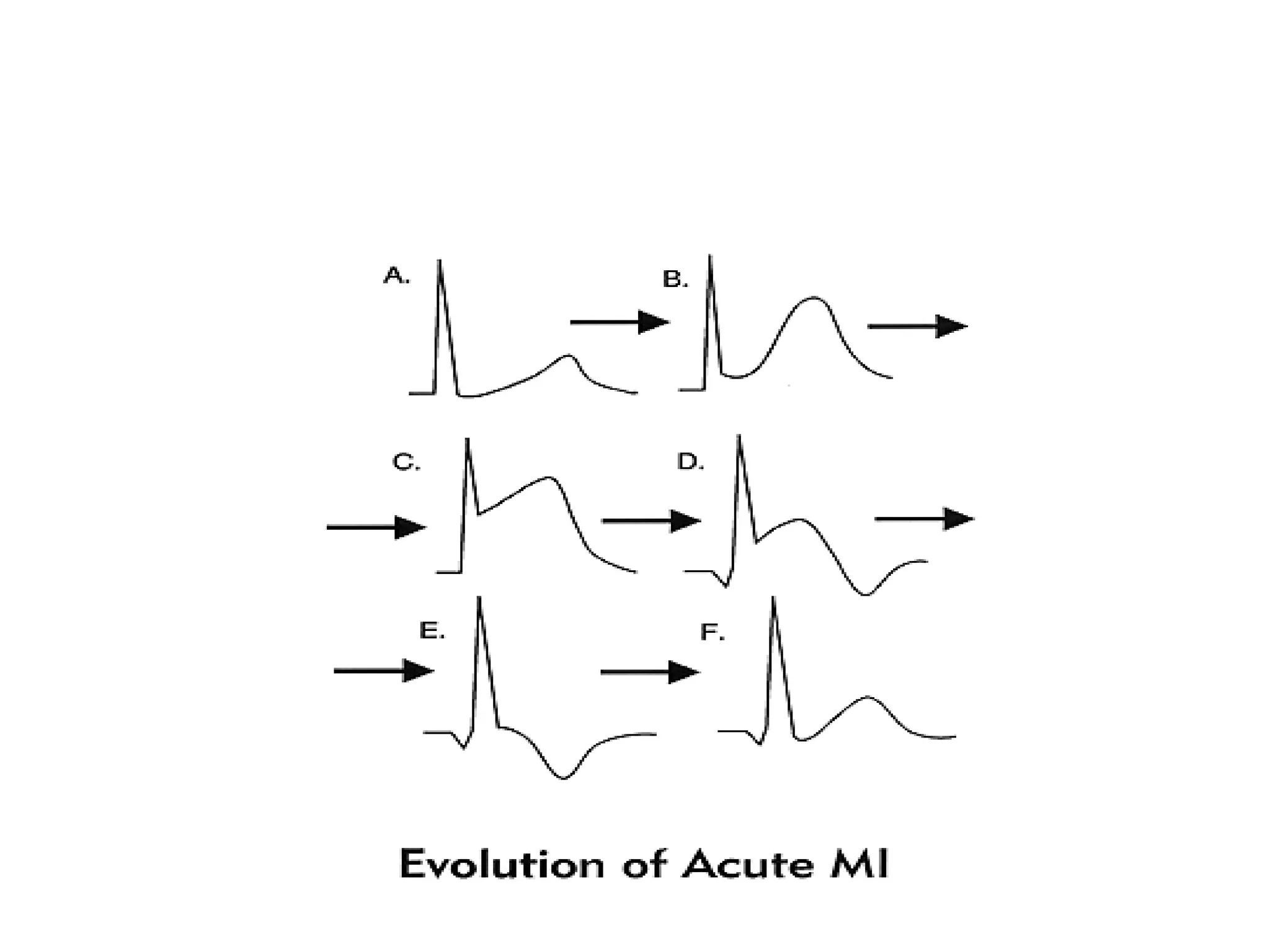



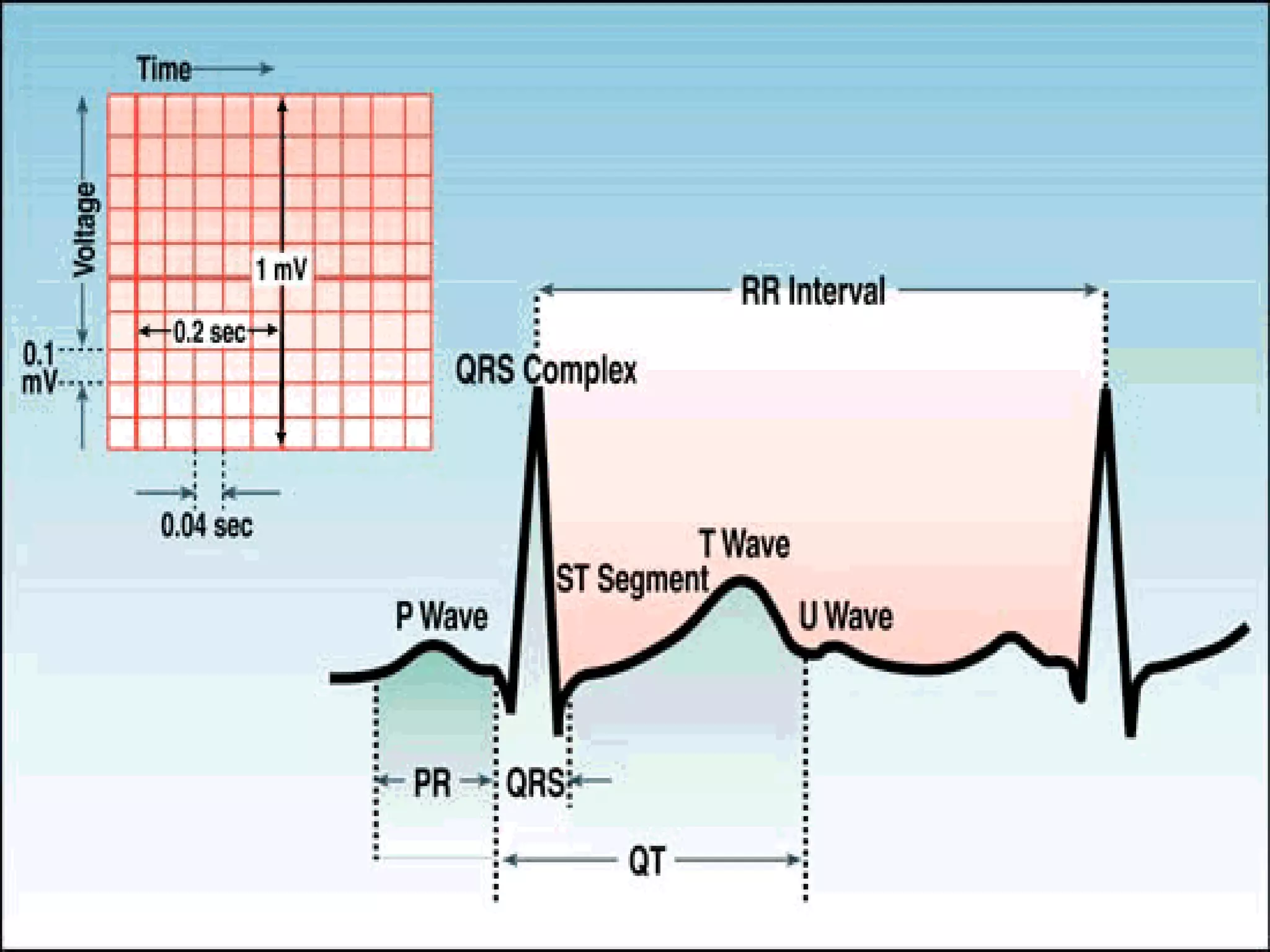







The ECG measures the electrical activity of the heart. Each component of the ECG waveform provides important information about the heart's structure and function. Abnormalities seen on the ECG can help identify arrhythmias, conduction defects, chamber enlargement, ischemia, infarction and other cardiac pathologies. A thorough understanding of normal ECG patterns is required to accurately interpret ECG tracings and diagnose cardiac conditions.







































































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)


