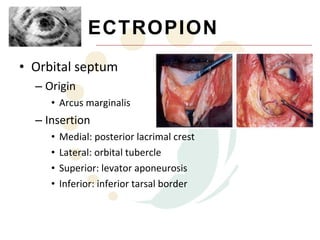
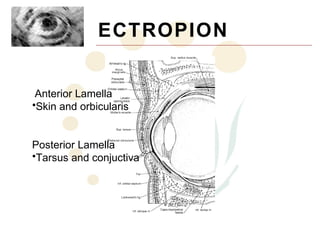
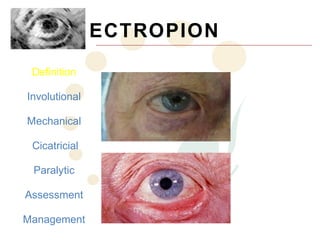
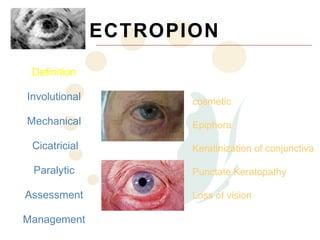
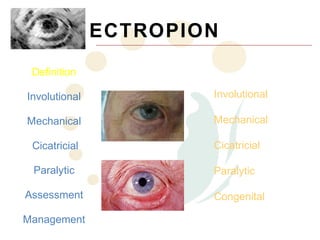
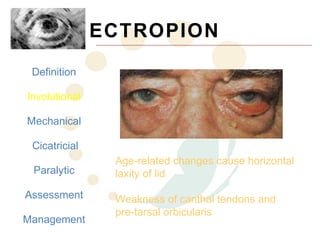
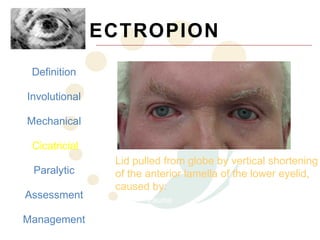
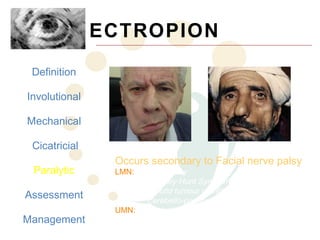
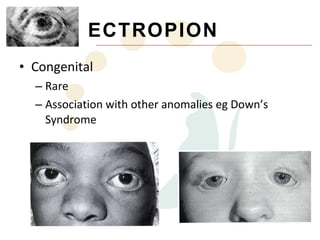
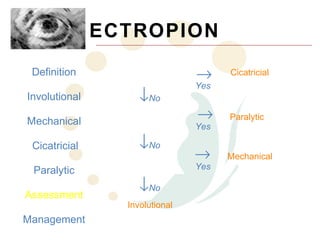
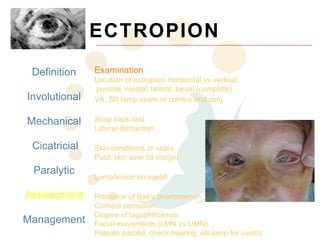
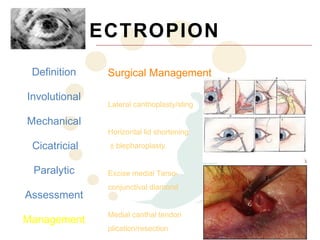
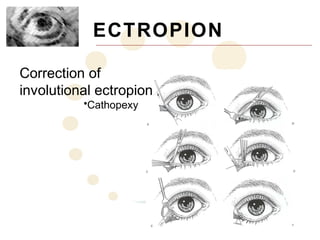
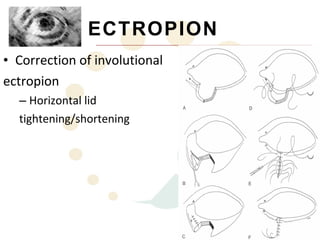
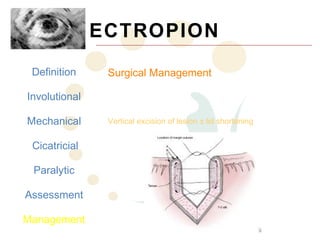
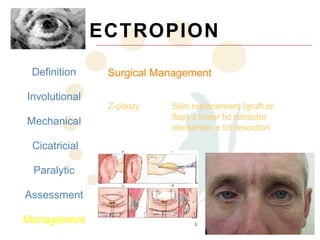
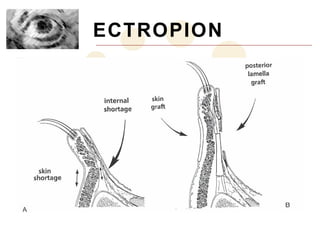
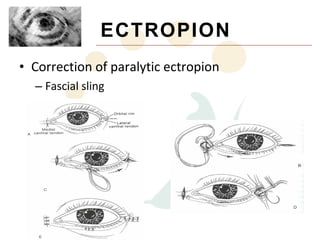
Ectropion is the abnormal eversion of the eyelid away from the globe. It can be involutional, mechanical, cicatricial, or paralytic in nature. Examination involves assessing for corneal exposure, lid laxity, lesions, and facial nerve function. Management includes lubricants, taping, scar massage, and various surgical techniques depending on the underlying cause such as lateral tarsal strip surgery for involutional ectropion or fascial sling for paralytic ectropion.