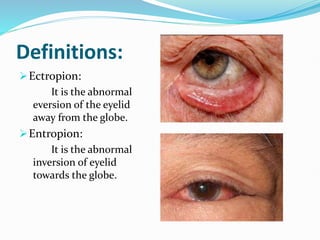
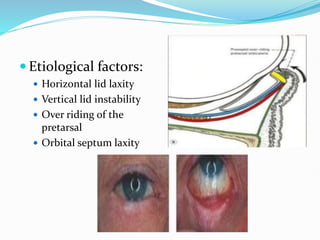
1. Ectropion and entropion are abnormal positions of the eyelid that can cause irritation and damage to the eye. Ectropion involves eversion of the eyelid away from the eye, while entropion involves inversion of the eyelid toward the eye.
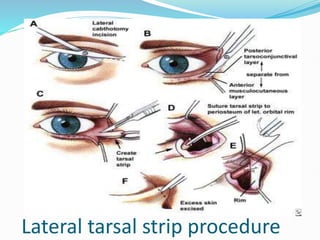
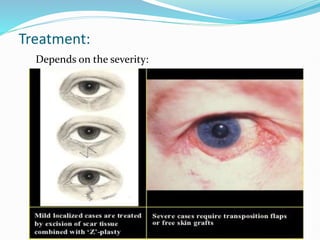
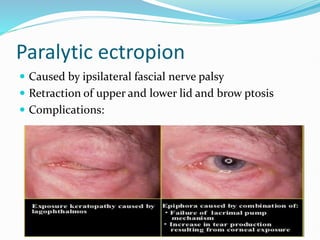
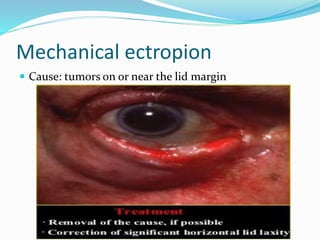
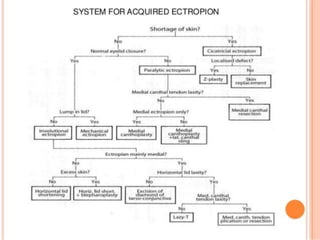
2. Causes of ectropion include aging, nerve palsy, scarring from burns or surgery, herniated fat or eyelid tumors, allergies, and congenital abnormalities. Treatment depends on the cause and location, and may include lateral tarsal strip procedure, pentagon excision, or medial spindle procedure.
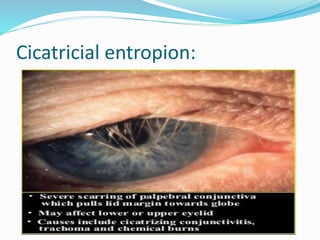
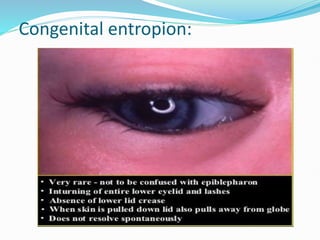
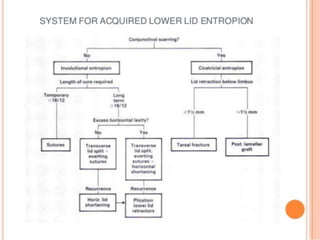
3. Entropion is usually caused by aging which results in tissue lax