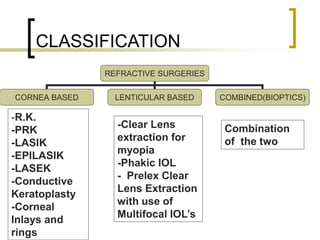
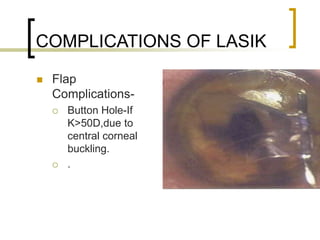
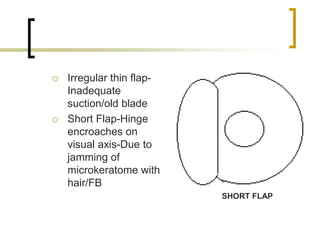
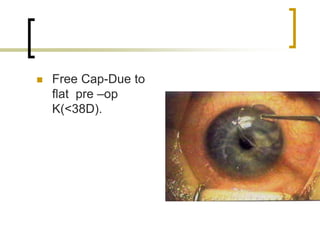
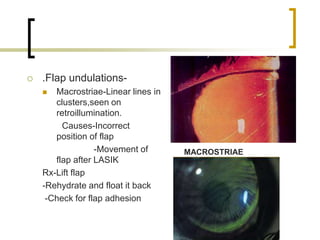
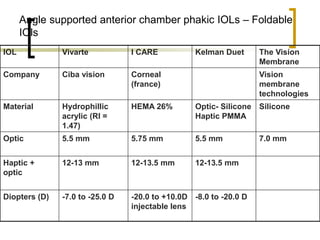
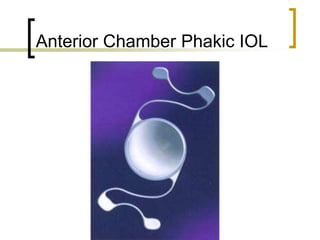
This document provides information on various refractive surgeries including classification, procedures, and complications. It discusses corneal-based procedures like LASIK, PRK, LASEK, conductive keratoplasty, and corneal inlays. It also discusses lenticular-based procedures like clear lens extraction and phakic IOLs, as well as combined/bioptic procedures. Details are provided on the LASIK procedure, patient selection criteria, contraindications, and potential complications. Other refractive surgery options like conductive keratoplasty, corneal inlays, and phakic IOLs are also summarized.