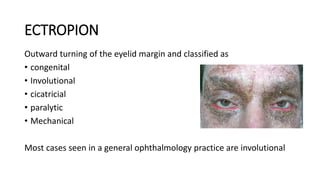
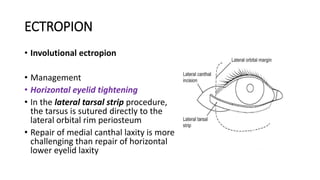
This document summarizes various periorbital malpositions and involutional changes including ectropion, entropion, and symblepharon. Ectropion is outward turning of the eyelid and has several types including involutional, cicatricial, and paralytic. Entropion is inward turning and can be involutional, acute spastic, or cicatricial. Symblepharon is an adhesion between conjunctival surfaces caused by inflammation, infection, or trauma. The document discusses examination, risk factors, pathophysiology, and management options for each condition including surgical procedures and medical treatment.