Downloaded 66 times
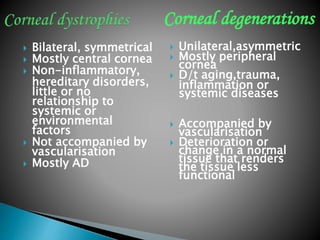
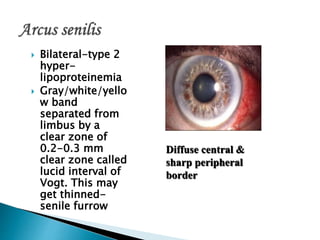


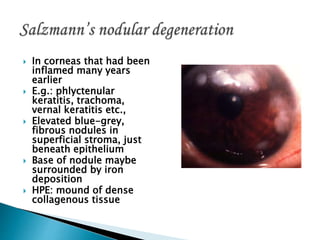




This document discusses various types of corneal degenerations and dystrophies. It provides descriptions of conditions such as arcus senilis, band keratopathy, corneal dystrophies, and corneal depositions. The causes, characteristics, associated systemic diseases, histopathological features, and treatments are summarized for each condition.








































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)














