Case Presentation: Duane's Syndrome
•Download as PPTX, PDF•
14 likes•14,435 views

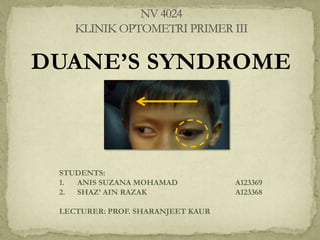
The document describes a case of Duane's syndrome in a 10-year-old male patient. Clinical findings showed limitation of adduction and globe retraction of the left eye, consistent with Duane's syndrome type 2. Refraction found low myopia and astigmatism, causing reduced vision. The patient was prescribed glasses and referred to a hospital for further evaluation and possible surgery due to a marked alternating head posture. Duane's syndrome is a congenital eye movement disorder caused by abnormal innervation of the eye muscles.

More Related Content
What's hot
What's hot (20)
Similar to Case Presentation: Duane's Syndrome
Similar to Case Presentation: Duane's Syndrome (20)
More from Anis Suzanna Mohamad
More from Anis Suzanna Mohamad (20)
Recently uploaded
Recently uploaded (20)
Case Presentation: Duane's Syndrome
- 1. DUANE’S SYNDROME STUDENTS: 1. ANIS SUZANA MOHAMAD 2. SHAZ’ AIN RAZAK LECTURER: PROF. SHARANJEET KAUR A123369 A123368
- 2. DUANE’S SYNDROME aka Duane’s retraction syndrome a congenital eye movement disorder due to misdirection of the nerve fibre on eye muscle causing some eye muscle to contract when they shouldn’t, vice versa can be unilateral or bilateral
- 3. Aetiology: 1. Mechanical factors fibrosed LR abnormally insertion of MR binding of MR sheath to wall 2. Embryonic factors Disturbance in normal embryonic development during 2nd month of gestation 3. 4. Development of 3rd, 4th, and 6th cranial nerve occur Paradoxical innervation Increase innervation to both MR & LR during ADD and relaxation of both MR & LR during ABD Trauma
- 4. Clinical features: limitation of abduction with or without limitation of adduction attempt adduction: retraction of the globe with narrowing of fissure Protrusion & widening of the palpebral fissure on abduction May or may not have AHP Strabismus Amblyopia
- 5. PATIENT: MALE/10/MALAY FILE NO: 0377 Date: 28th February 2012 CHIEF COMPLAINT -complaint of blur when seeing distance, want to make spectacles -has problem in writing ; words become shuffle since kindergarten OCULAR HISTORY -Father claimed has lazy eye since 2-3 years old, has follow up at Hosp. Terengganu -easily fall when young, suspect due to lazy eye -wear spect at very young age but refused to wear till now GENERAL -Asthma, eczema, use homeopathy FAMILY HISTORY -Mother has DM, HPT since 8mo ago
- 6. RE VA *with marked AHP : face turn R LE 6/12 PH: 6/9+ N5 @ 15cm PRIMARY GAZE 6/24 Not able to read Snellen on primary gaze AHP D N moderate XP PRIMARY GAZE COVER TEST 6/24 PH: 6/18+2 N5 @ 15cm D N large L XT HIRSCHBERG central Reflex at nasal AA 13,13,13 13,13,13 NPC 11cm LE deviates out STREOPSIS 240 arc (TNO) *not reliable
- 8. 1. LE Exotropia on primary gaze 2. V pattern LE has no problem when attempt on abduction (towards temporal) 3. Abduction on elevation: normal Abduction on depression: normal LE has limitation on adduction (towards nasal) 4. Down shooting of LE on adduction Also limitation of adduction on elevation & adduction on depression LE presents narrow palpebral fissure, and globe retraction on adduction
- 9. RE Limitation of ADDUCTION of LE 2. Down shoot of LE 1. *classic presentation of Duane’s Type 2 LE
- 10. RE LE KERATOMETRY 40.82@180 44.67@90 CA: -3.75x180 40.82@180 43.82@90 CA: -3.00x180 RETINOSCOPY PL/-4.00X15 6/12-2 -1.25/-0.75X170 6/12 SUBJ. RX -0.50/-3.00X10 6/9 -0.50/-1.75X170 6/9 OPHTHALMOSCOPY cd ratio: 0.5 A/V: 2/3 cd ratio: 0.6 A/V: 2/3
- 11. DIAGNOSIS 1. Low myope moderate astig 2. L Duane’s syndrome MANAGEMENT 1. Prescribe Rx 2. Write referral letter to Hosp. Terengganu 3. Refer pt to BV clinic for further assessment - 9 Apr 2012 4. KIV AA with Rx
- 12. The major complaint that pt has is blur at distance More specific- since when? is it sudden or gradually blur? Father claimed has lazy eye since young, should wear glasses but refuse could be related to chief complaint : blur- possible uncorrected refractive error The reason of failure wear glasses? Ask more about symptoms of amblyopia. Any eye turning in? Eye rubbing? See at very close distance?
- 13. DISCUSSION: CLINICAL FINDINGS Reduction in vision BE 1. Improvement with pinhole: reduction of vision can be corrected with spectacles However vision is taken with marked AHP Visual acuity with head straight shows further decrement in vision on LE Marked AHP- face turn R 2. Visual acuity is better on LE however marked large exo-deviation on LE in primary position face turn R (non deviating side) is significant as to obtain fusion.
- 14. AHP • Left exotropia. As face turn to right (non affected side), it will compensate the deviation. • To improve visual acuity • To decrease deviation, hence strengthen BSV. Cover test shows moderate XP with AHP compared to primary gaze PRIMARY GAZE FACE TURN RIGHT FACE TURN RIGHT
- 15. Refractive error 4. Unaided VA RE 6/24 is correlate with refraction finding -0.50/-3.00DCx10 (estimated astigmatism ~±3.00DC). Unaided VA LE 6/12 is correlate with refraction finding -0.50/-1.75X170 (estimated astigmatism ~±1.25DC). Most astigmatism power comes from corneal astigmatism. BE develop meridional amblyopia (6/9 BE) due to uncorrected astigmatism.
- 16. Diagnosis 1: low myope with moderate astig 1. Uncorrected moderate amount of astig presenting with reduce of vision Should suggest meridional amblyopia? Management: prescribe Rx to provide optimum correction & prevent moderate amblyopia Diagnosis 2: Left Duane’s syndrome 2. Limitation of adduction on LE On attempt of adduction, affected eye appear smaller (palpebral fissure narrowing, globe retraction), and down shoot. Classic sign on Duane’s Type 2. There is 4 types of Duane’s syndrome Management: refer to Hospital and BV clinic
- 17. Refer to BV: patient came on 2nd April 2012 Additional test- Hess chart: to investigate incomitant strabismus in order to asses paretic element LE 1. LE has smaller field than RE. Suggest LE affected eye. 2. Sloping sides to field indicates V pattern. 3. Compressed field of LE on nasal part. • Underaction of Left MR, IO, SO 4. Larger field of RE • Overaction of Right SR, LR, IR RE
- 18. TYPE 1 TYPE 2 TYPE 3 TYPE 4 -Poor abduction, good adduction -Poor adduction, good abduction -Poor adduction, poor abduction -Paradoxical abduction on attempt adduction -agenisis of 6th nerve -3rd nerve split innervate LR, MR -adduction intact as most nerve goes to MR -6th nerve intact -3rd nerve split innervate LR, MR -Poor adduction as LR contract against MR -6th nerve agenesis -3rd nerve split innervate LR, MR -The split is equal -Eye not moves in/out -6th nerve agenesis -3rd nerve split innervate LR, MR -most innervate LR -when ADD it ABD
- 19. TYPE 1 (70-80%) ie: LE LE Esotropia with head straight Face turn to affected side TYPE 2 (~7%) ie: LE LE Exotropia with head straight TYPE 3 (~15%) TYPE 4 ie: LE Eyes are aligned in primary position with head straight ie: LE Large LE Exotropia Face turn to nonaffected side Limited abduction left eye Normal or less abduction -Normal or less adduction -Narrowing of fissure -Globe retraction -Limited adduction -Narrowing of fissure -Globe retraction -Marked upshoot and sometimes downshoot on adduction Limited abduction left eye -Limited adduction -Narrowing of fissure -Globe retraction -Upshoot/ down shoot Limited adduction RE Simultaneous abduction when looking toward uninvolved side -violating Hering’s law
- 20. Management of Duane’s syndrome Correct refractive error Treat amblyopia In this case, no patching treatment is indicated yet as vision BE is almost similar Meridional amblyopia usually has good prognosis with spectacles alone To monitor vision after correction after 3 months. Surgery indicated if: Marked AHP Decompensating Cosmetically poor deviation Diplopia occurring more frequently
- 21. Refer to ophthalmology To perform additional test for further evaluation Forced duction test: to evaluate muscle palsy (+ve forced duction test) Suggestion for squint surgery The marked AHP is consistent To improve cosmesis & comfort to patient
- 22. Duane’s syndrome is a congenital eye movement disorder in which there is miswiring of the eye muscles that typically can be recognized through a few ocular signs and symptoms. As an optometrist, we should smartly recognized this syndrome according to the history taking and clinical findings in order to make an accurate diagnosis. Although the syndrome is permanent, further managements is crucial in order to solve patient’s problems such as marked AHP and also on.
- 23. 1. Fiona J. Rowe. Clinical orthoptics. 3rd edition. 2. 3. 4. 5. Wiley-blackwell. http://emedicine.medscape.com/article/119855 9-overview date: 20th April 2012 http://telemedicine.orbis.org/bins/volume_page. asp?cid=1-3-5-50 date: 20th April 2012 http://www.webmd.com/eye-health/duanesyndrome date: 20th April 2012 http://childrenshospital.org/az/Site3103/mainpa geS3103P0.html date: 20th April 2012
- 24. Thank You
Editor's Notes
- Duane syndrome: A congenital eye movement disorder in which there is miswiring of the eye muscles, causing some eye muscles to contract when they should not and other eye muscles not to contract when they should. People with the syndrome have a limited (and sometimes no) ability to move the eye outward toward the ear (to abduct the eye) and, in most cases, a limited ability to move the eye inward toward the nose (to adduct the eye). Often, when the eye moves toward the nose, the eyeball also pulls into the socket (retracts), the eye opening narrows and, in some cases, the eye moves upward or downward. Many patients with Duane syndrome turn their face to maintain binocular vision and compensate for improper turning of the eyes.
- Bluring of vision at distance suggest uncorrected refractive errorHas significant ocular history regarding Should ask more the condition of blur vision. -Is it gradually decrease/ becoming worse or persistent blur vision?-
- Reduction in vision BE-Improvement with pinhole: part of reduction of vision can be corrected with spectacles-However vision is taken with marked AHP-Visual acuity with head straight shows further decrement in vision on LE2. Marked AHP- face turn R -vision is better on LE -however marked large exo-deviation on LE. AHP: face turn R (non deviating side) is significant as to obtain fusion. Large L XT is correlate with corneal reflex displaced nasally and AHP: face turn to right.
- MRunderaction -4SO overaction +2
- 2. Marked AHP- face turn R -vision is better on LE -however marked large exo-deviation on LE. AHP: face turn R (non deviating side) is significant as to obtain fusion.
- Agenesis-