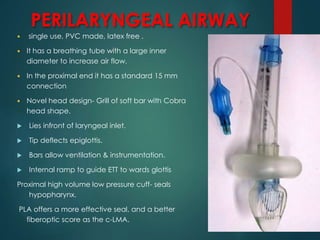
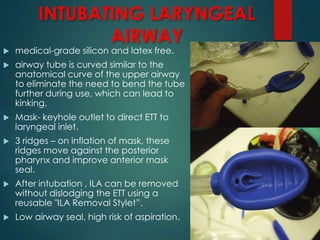
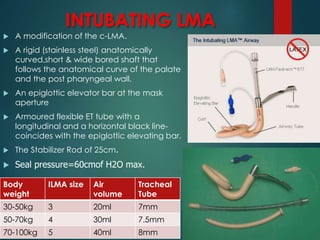
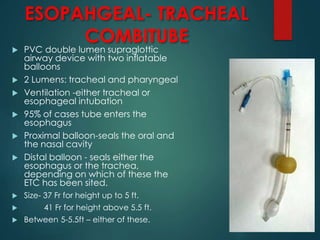
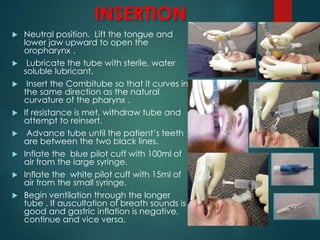
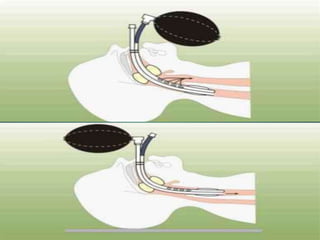
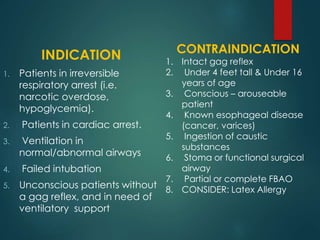
This document discusses supraglottic airway devices. It begins by introducing supraglottic airway devices as those that maintain airway patency by sitting above the glottic opening. It then classifies devices based on generation, sealing mechanism, number of lumens, and discusses indications, contraindications, advantages, and disadvantages of supraglottic airway devices. Specific devices like LMA Classic, Flexible LMA, Ambu Aura, Soft Seal LMA, and Intubating LMA are then described in more detail. Problems associated with devices and techniques to reduce aspiration are also covered.




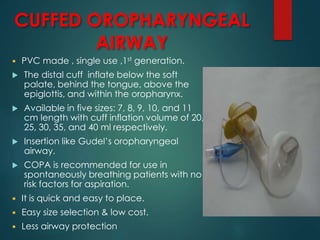

































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)












