Downloaded 70 times



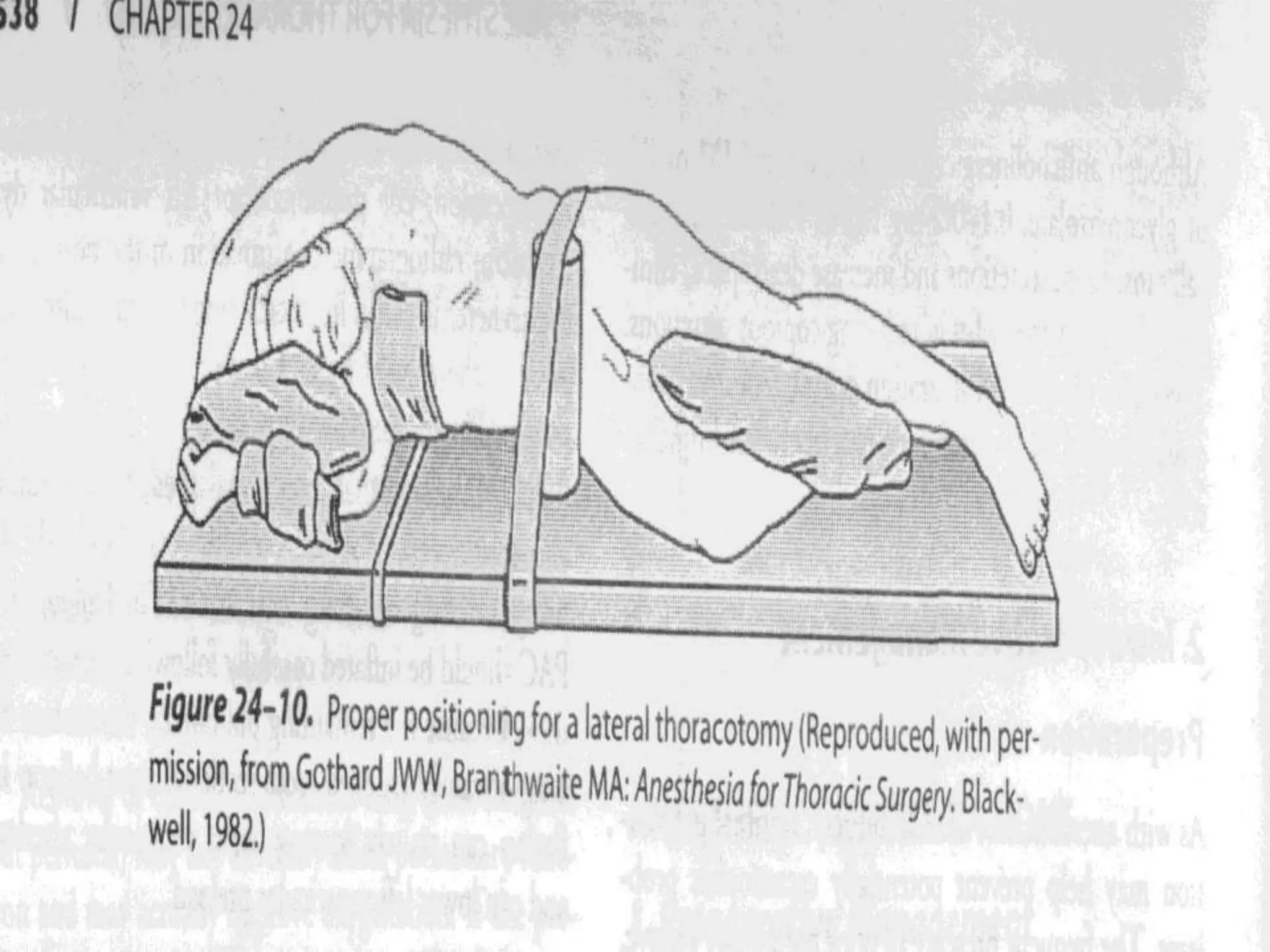

































































1) Thoracic anesthesia presents unique physiologic challenges including lung mechanics changes with lateral positioning, open pneumothorax risks, and one lung ventilation complications like hypoxic pulmonary vasoconstriction inhibition. 2) Careful patient evaluation and optimization is important preoperatively, including pulmonary function tests and cardiac evaluation. Intraoperatively, techniques like double lumen tubes, lung isolation, and thoracic epidural analgesia are utilized. 3) Postoperative complications can include pulmonary issues like edema, hemorrhage, or respiratory failure. Prolonged air leaks or bleeding may require chest tube insertion.























































































