Downloaded 428 times










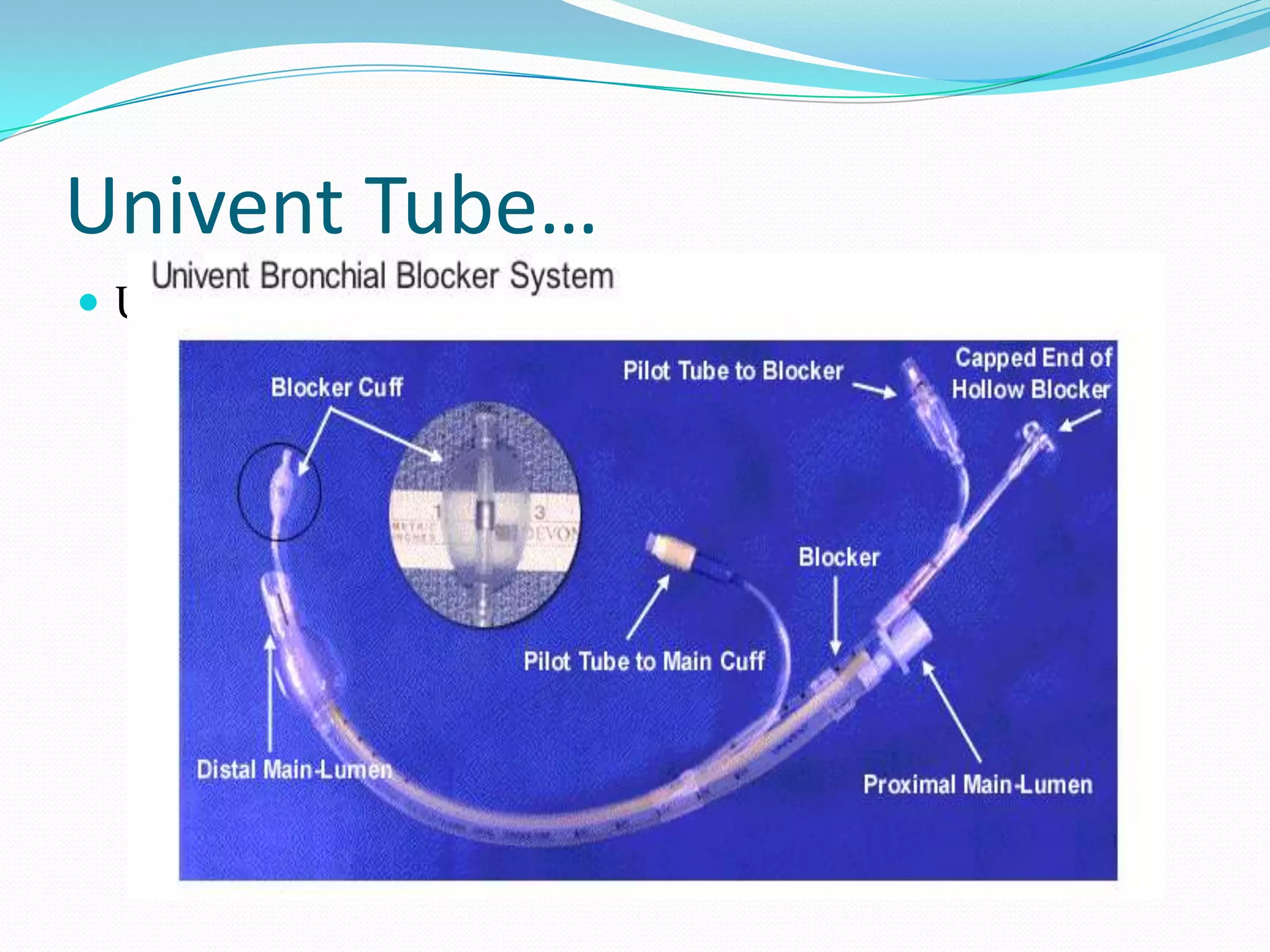













Bronchial blockers are inflatable devices that can be used to selectively isolate one lung during surgery by occluding a bronchial opening. They are indicated when a double lumen endotracheal tube cannot be used due to difficult airway, cervical spine injuries, or other anatomical issues. Common types of bronchial blockers include the Univent tube, Cohen bronchial blocker, Fogarty embolectomy catheter, and Arndt endobronchial blocker, each with their own advantages and limitations.























































































