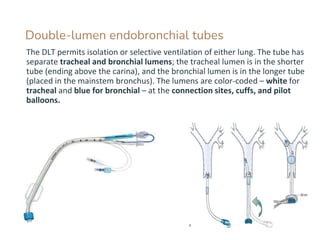
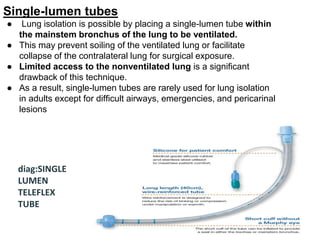
Lung isolation techniques are utilized to ventilate one lung during various surgical procedures, employing devices like double-lumen tubes (DLTs) and bronchial blockers. DLTs provide a preferential seal and ease of use during bilateral surgeries, while bronchial blockers are less invasive and associated with lower hemodynamic stress. However, single-lumen tubes are infrequently used for lung isolation in adults due to limited access to the nonventilated lung.