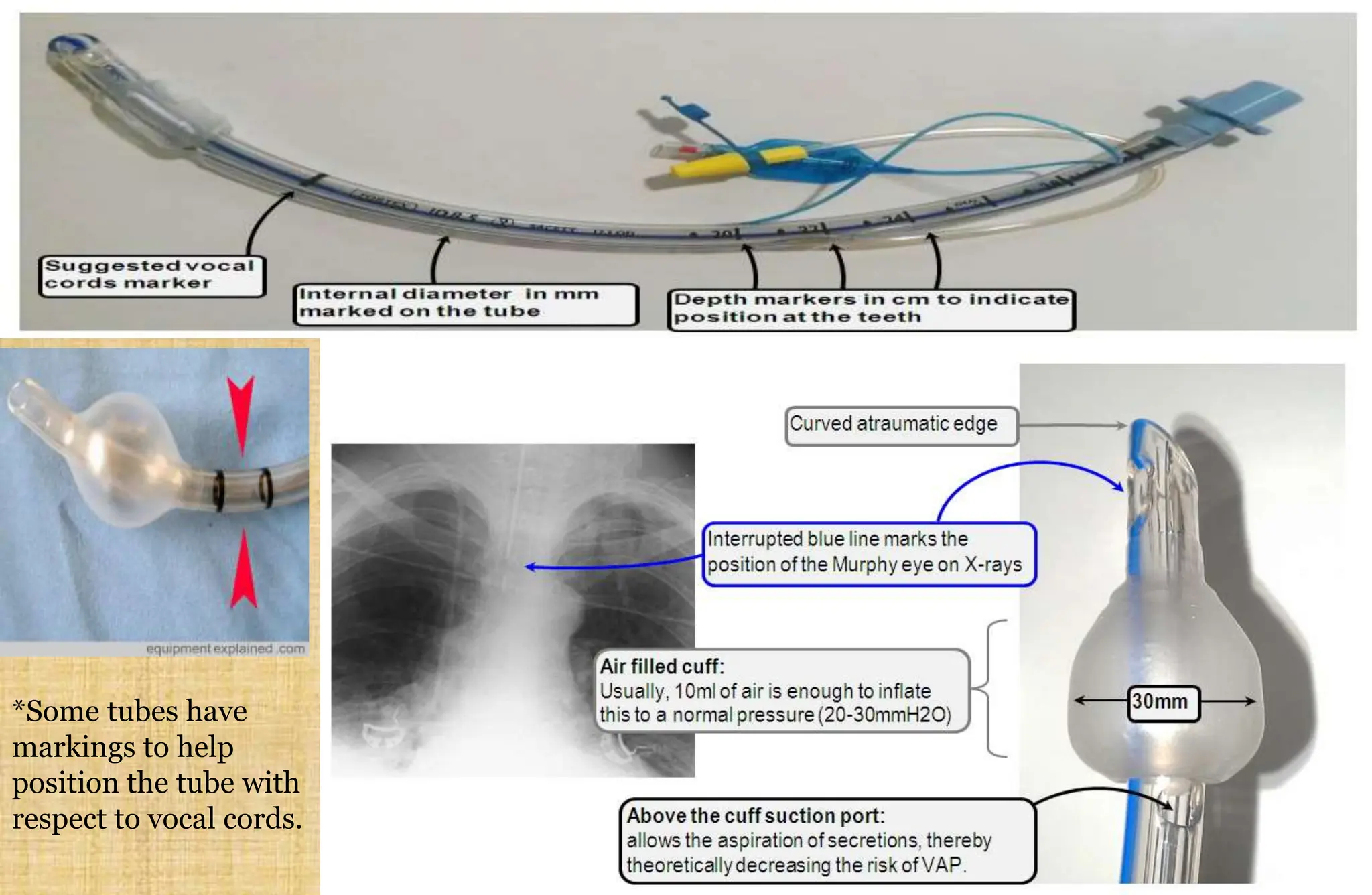
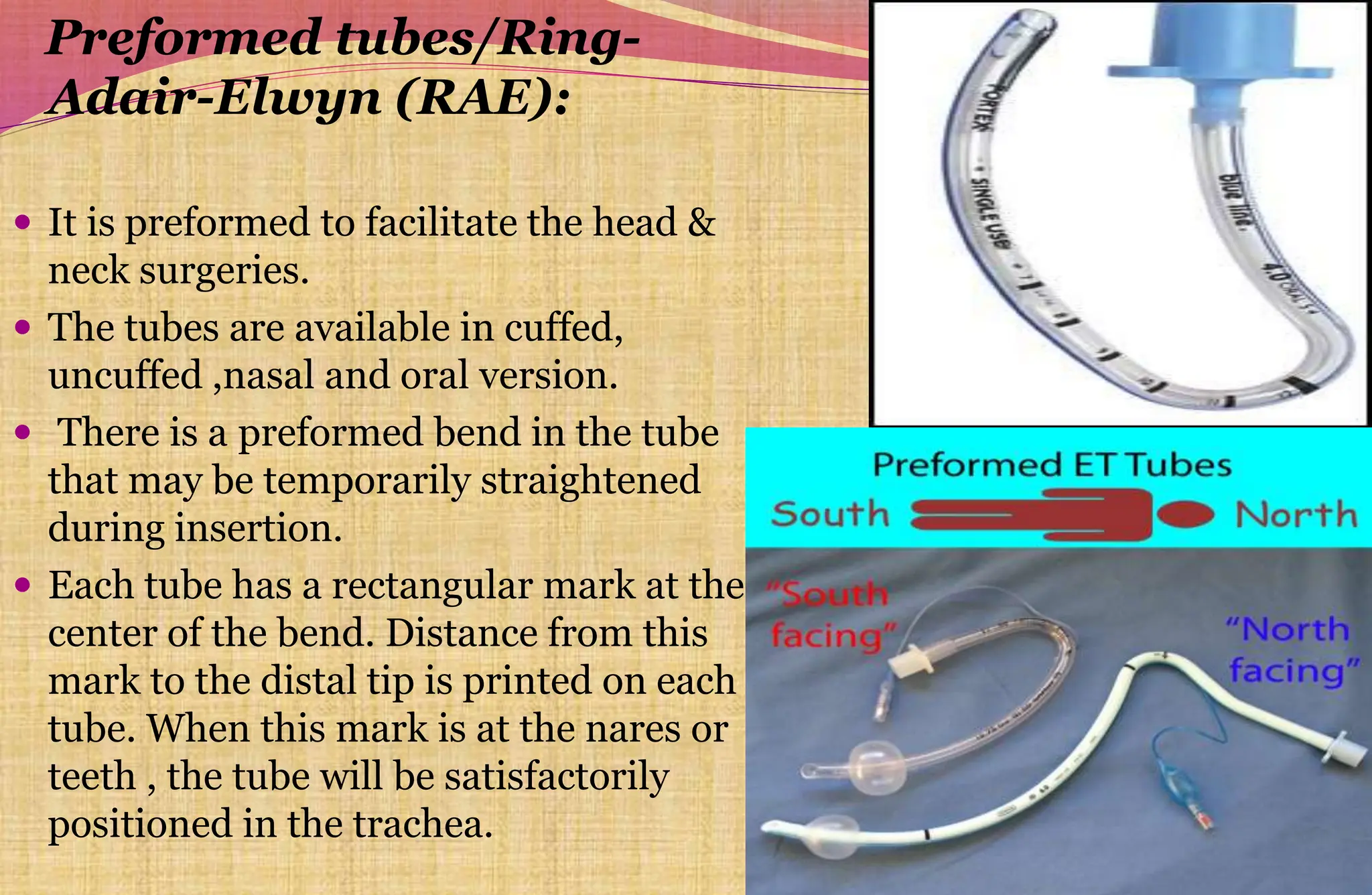
Endotracheal tubes are inserted into the trachea to allow for ventilation of the lungs. They come in various sizes and materials. Ideal tubes are low cost, inert, and have smooth surfaces. Complications can occur from intubation like trauma, esophageal insertion, or misplacement. Tube size is based on patient age, height, or finger size. Position must be confirmed before use to ensure proper lung ventilation and prevent aspiration. Specialty tubes are made for specific situations like head and neck surgeries.