This document discusses diabetic retinopathy, including:
- The two main types of diabetes and how they relate to retinopathy risk and onset age.
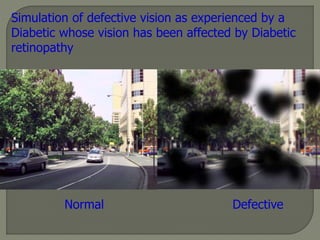
- Diabetic retinopathy as a leading cause of blindness and its impact.
- Key risk factors like diabetes duration, glycemic control, and other systemic factors.
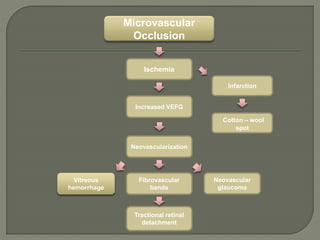
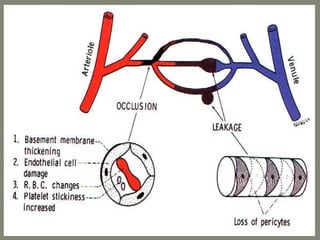
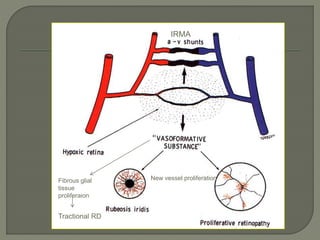
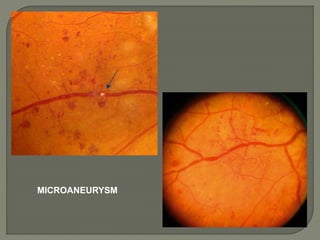
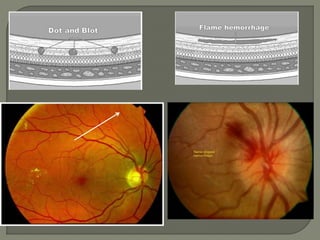
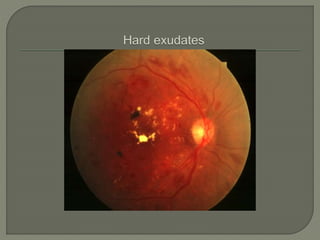
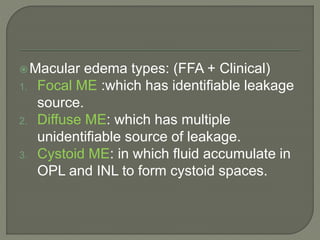
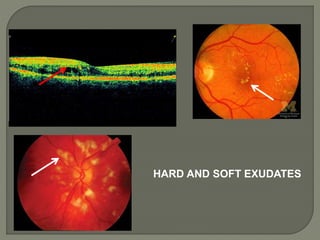
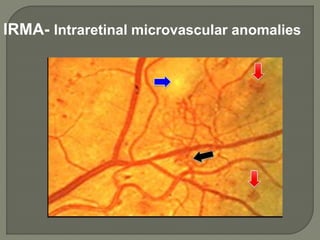
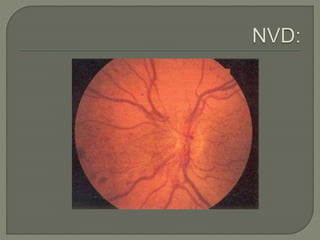
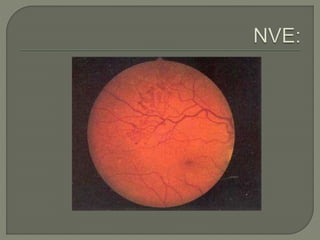
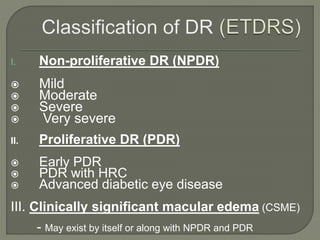
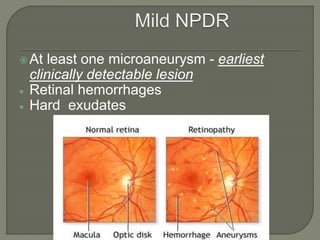
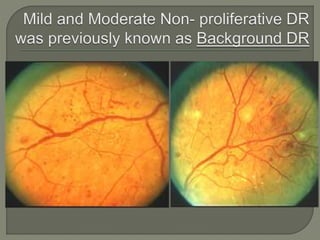
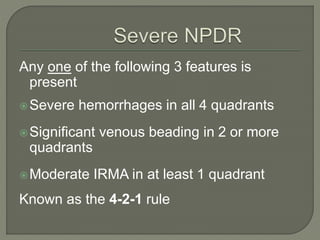
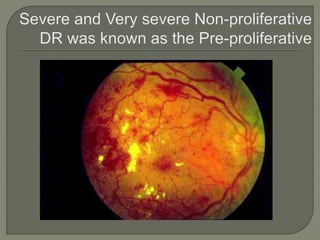
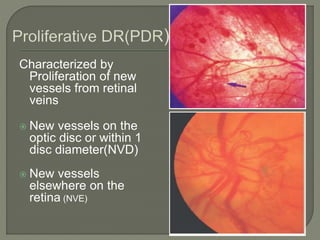
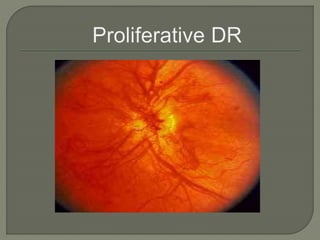
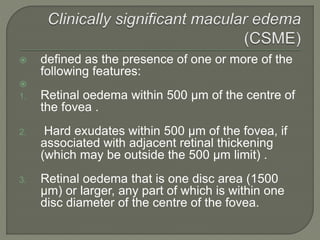
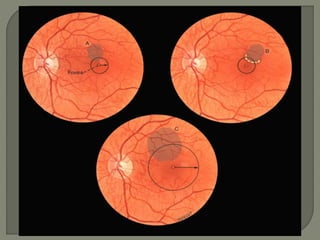
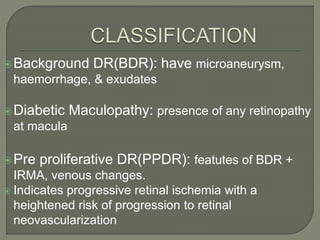
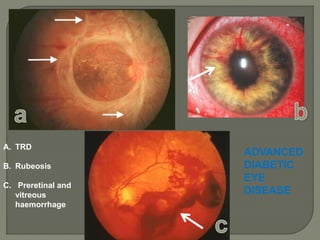
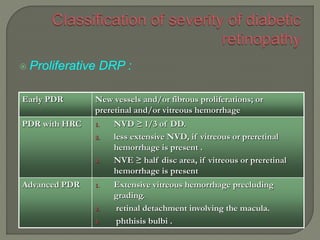
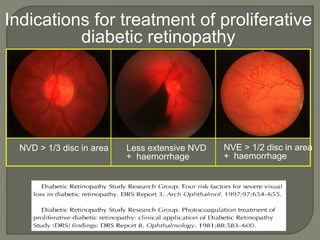
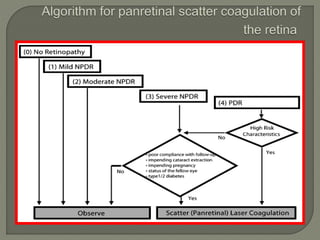
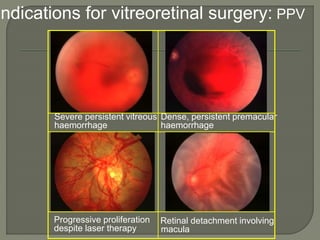
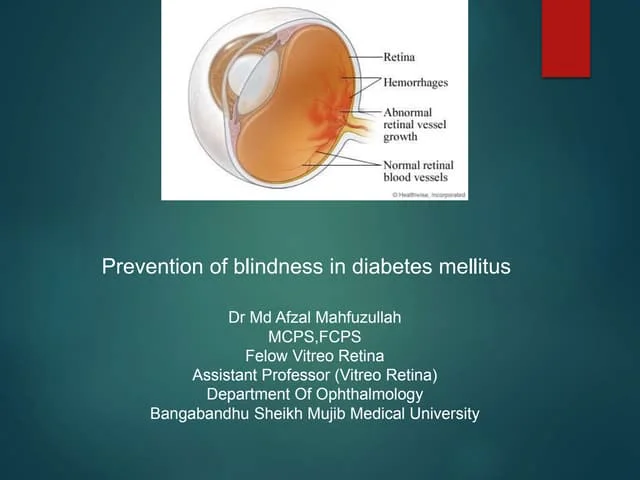
- The characteristic lesions and stages of non-proliferative and proliferative retinopathy.
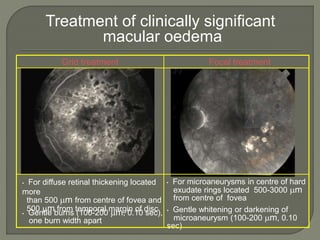
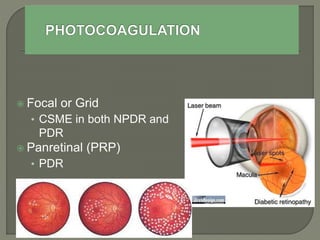
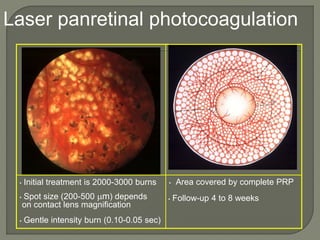
- Treatment approaches including laser photocoagulation, anti-VEGF injections, steroids, and surgery.
- Screening guidelines based on diabetes type and risk level.











































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)




![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)



