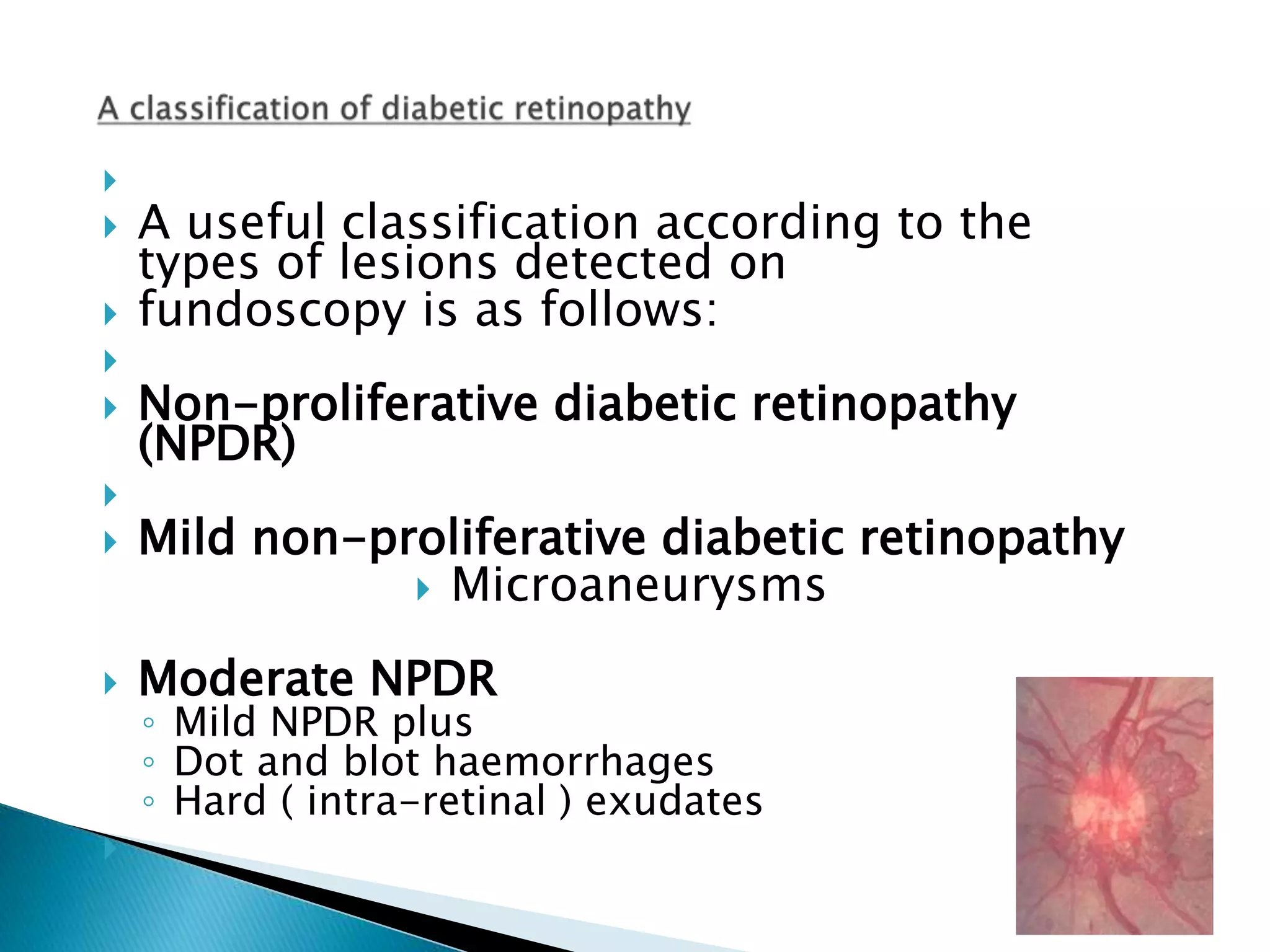
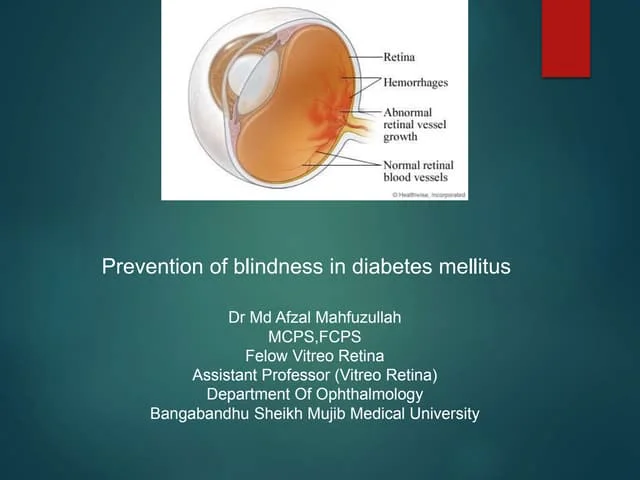
This document discusses diabetic retinopathy and its effects. It begins by noting the increasing prevalence of diabetes worldwide and that diabetes is a leading cause of blindness. It then describes the classification of diabetic retinopathy from mild non-proliferative to proliferative stages. Specific lesions associated with each stage are defined, including microaneurysms, hemorrhages, exudates, neovascularization, and retinal detachment. Risk factors for progression and visual loss from macular edema are also covered. The document emphasizes the importance of good blood sugar control in preventing and slowing the progression of diabetic retinopathy.