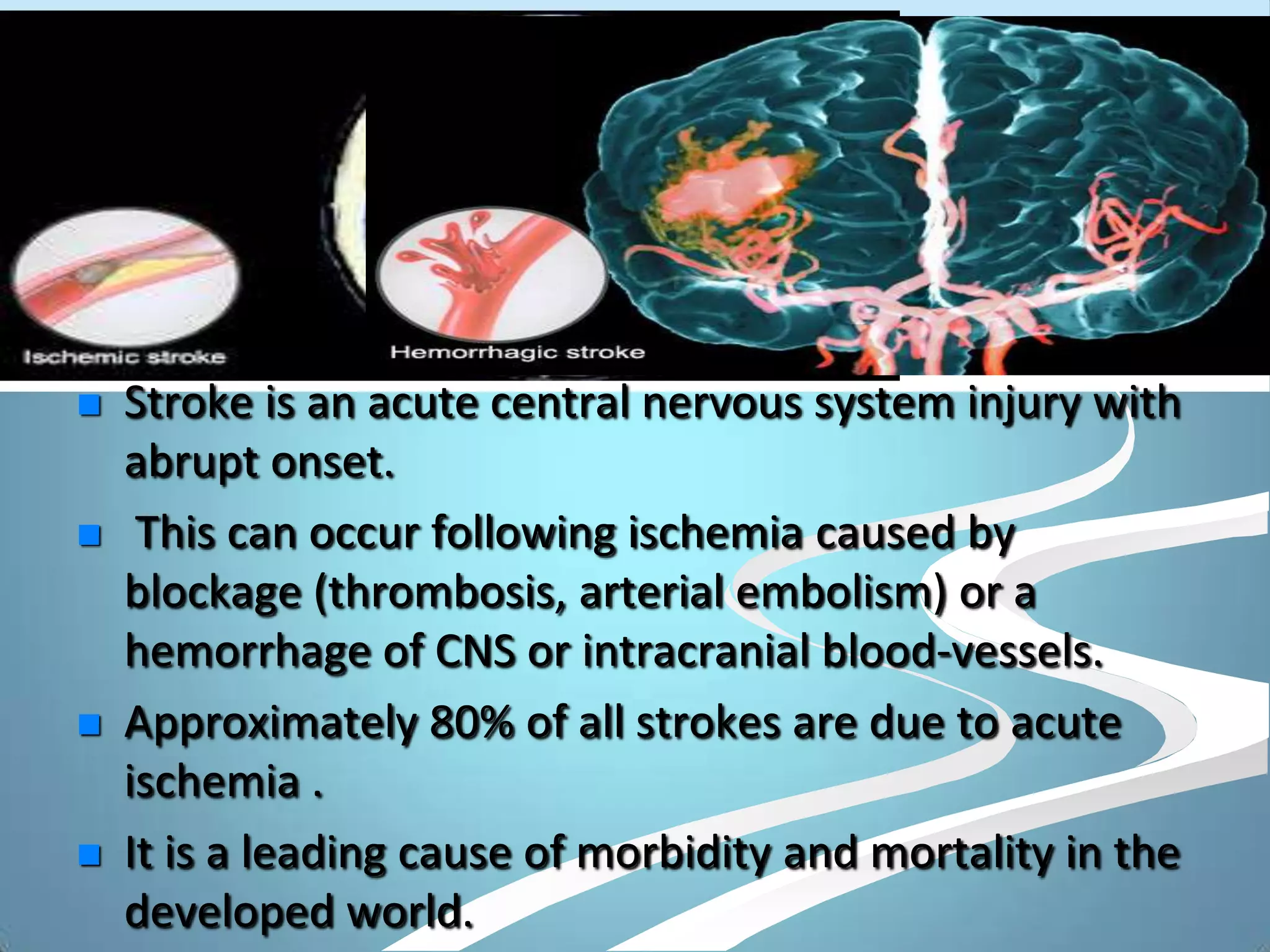
This document discusses various imaging modalities for stroke, focusing on their ability to assess the 4 P's: parenchyma, pipes, perfusion, and penumbra. CT techniques like non-contrast CT, CTA, and CTP can quickly detect hemorrhage, visualize vessels for clots, and assess perfusion/penumbra. MRI techniques like DWI, PWI, MRA provide highly sensitive visualization of acute ischemia and perfusion abnormalities to identify the ischemic core and penumbra. Imaging plays a crucial role in the early diagnosis and management of stroke by establishing the diagnosis, guiding therapy decisions, and identifying salvageable brain tissue.