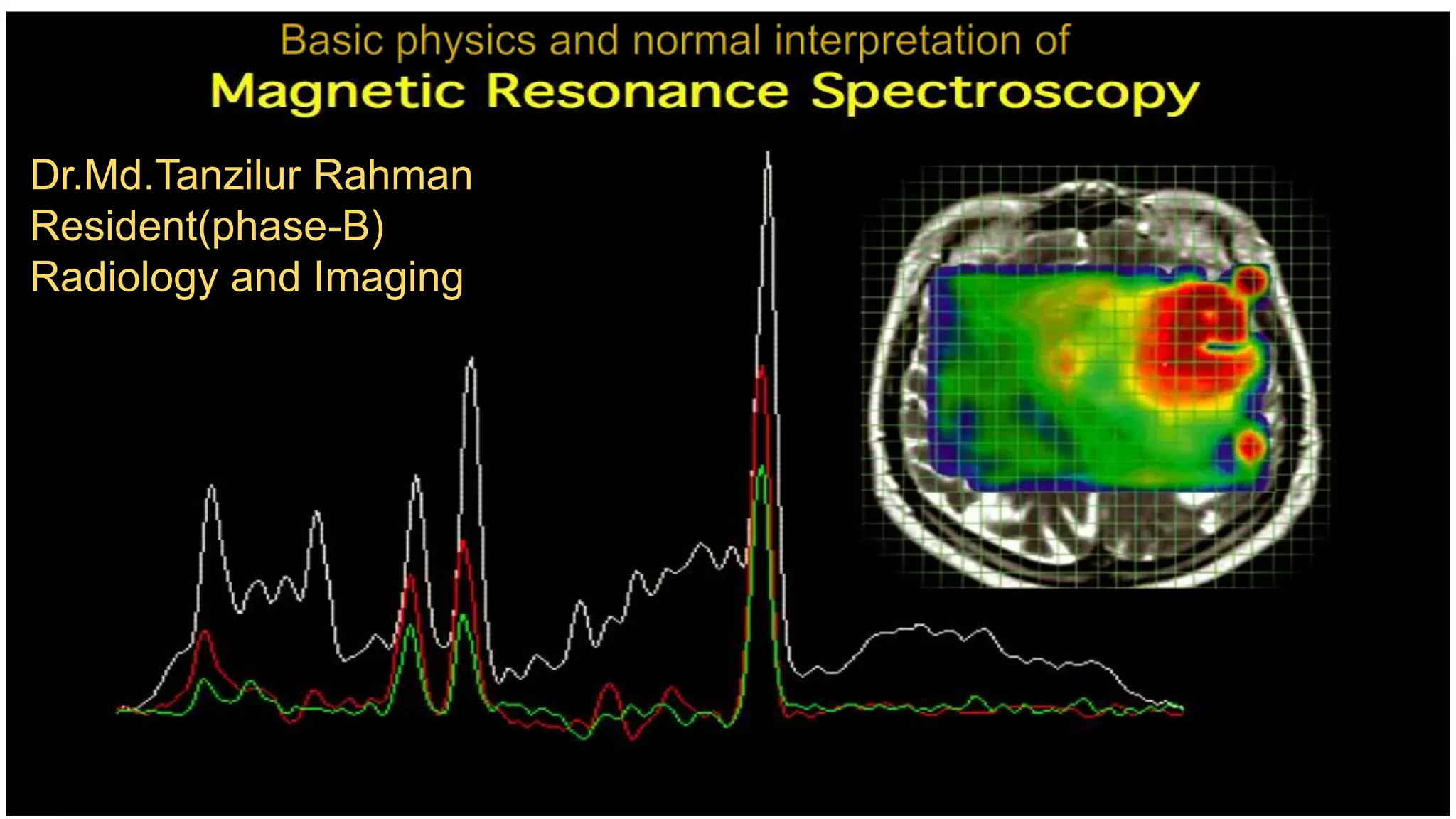
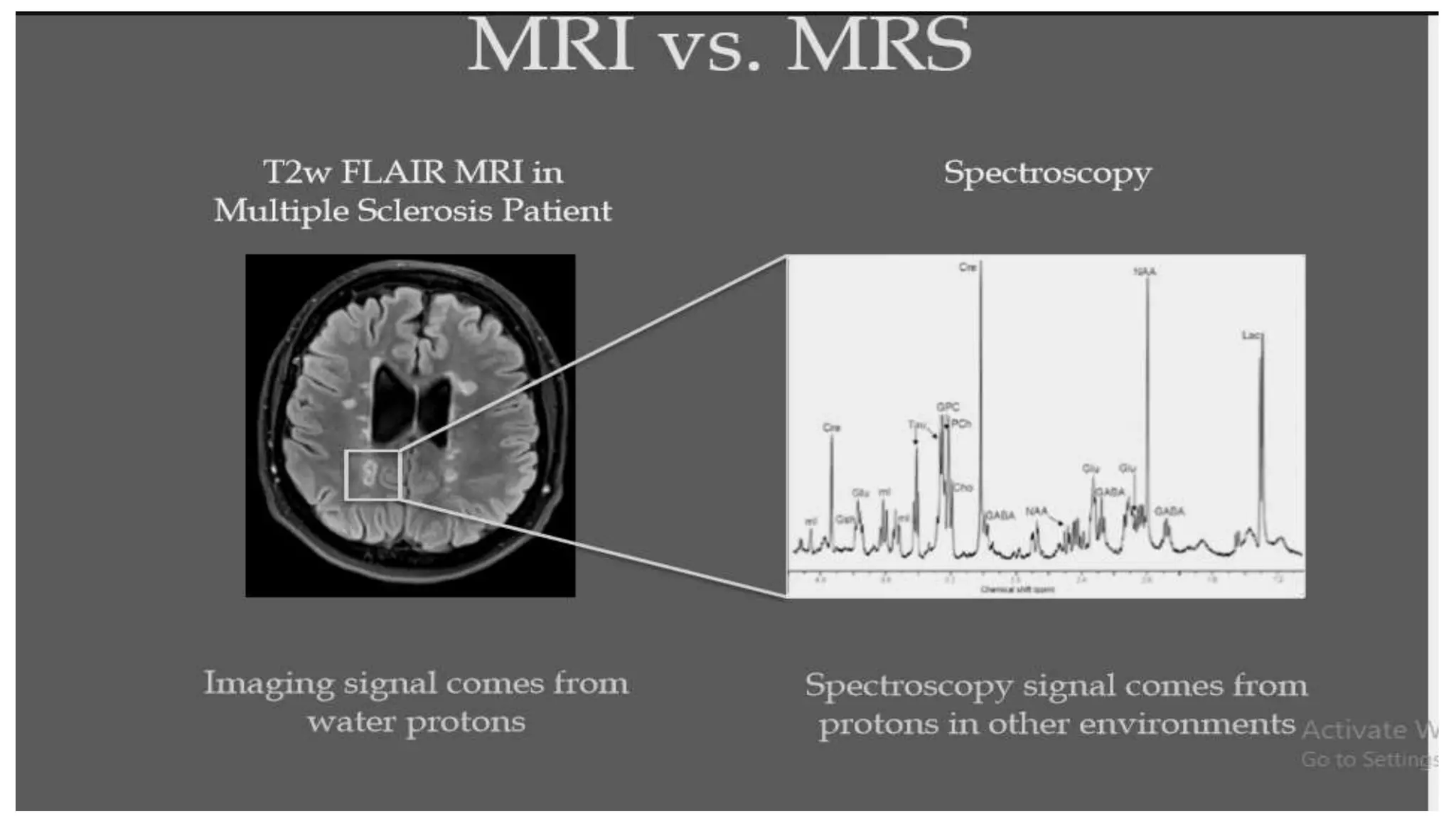
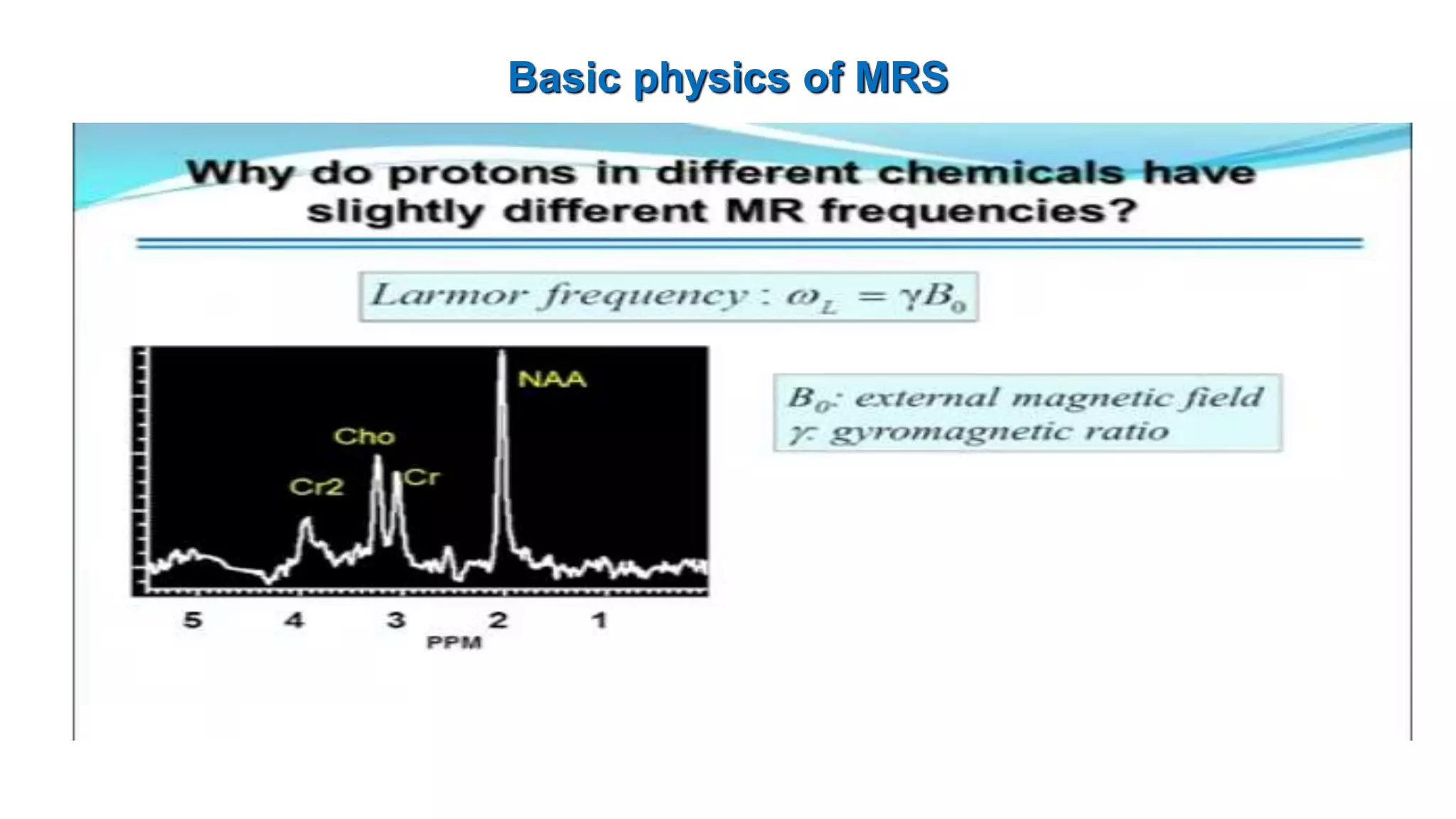
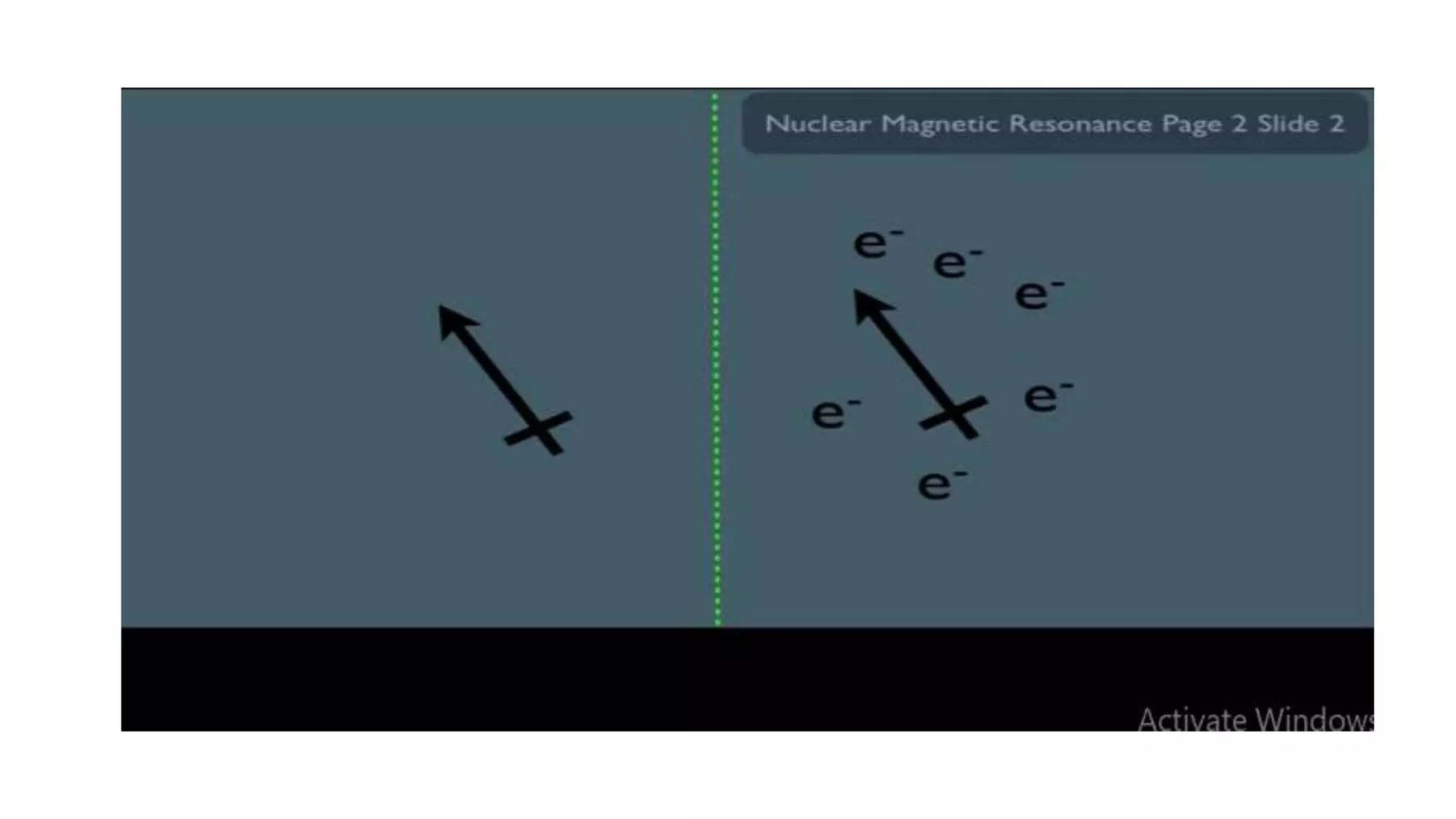
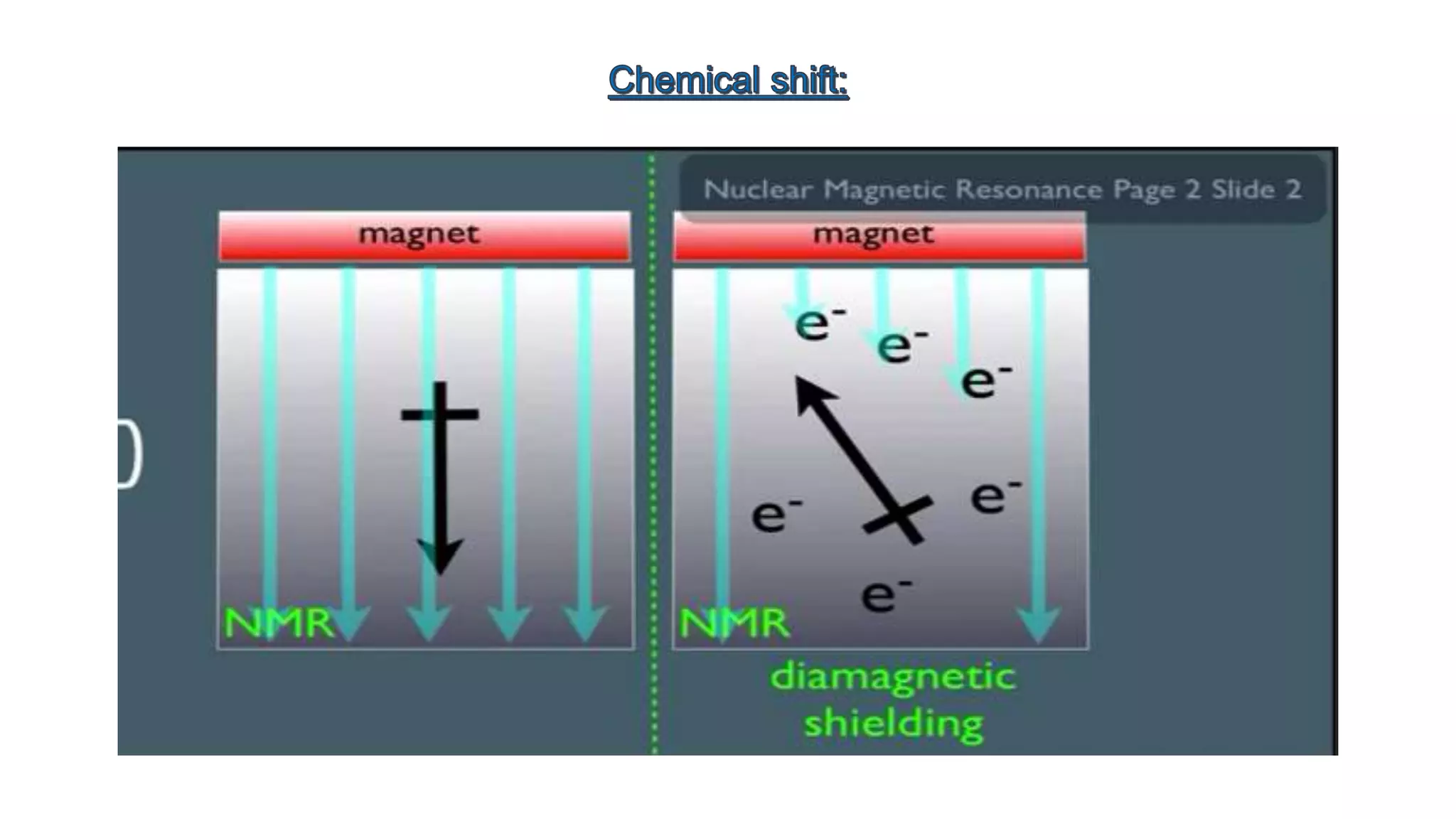
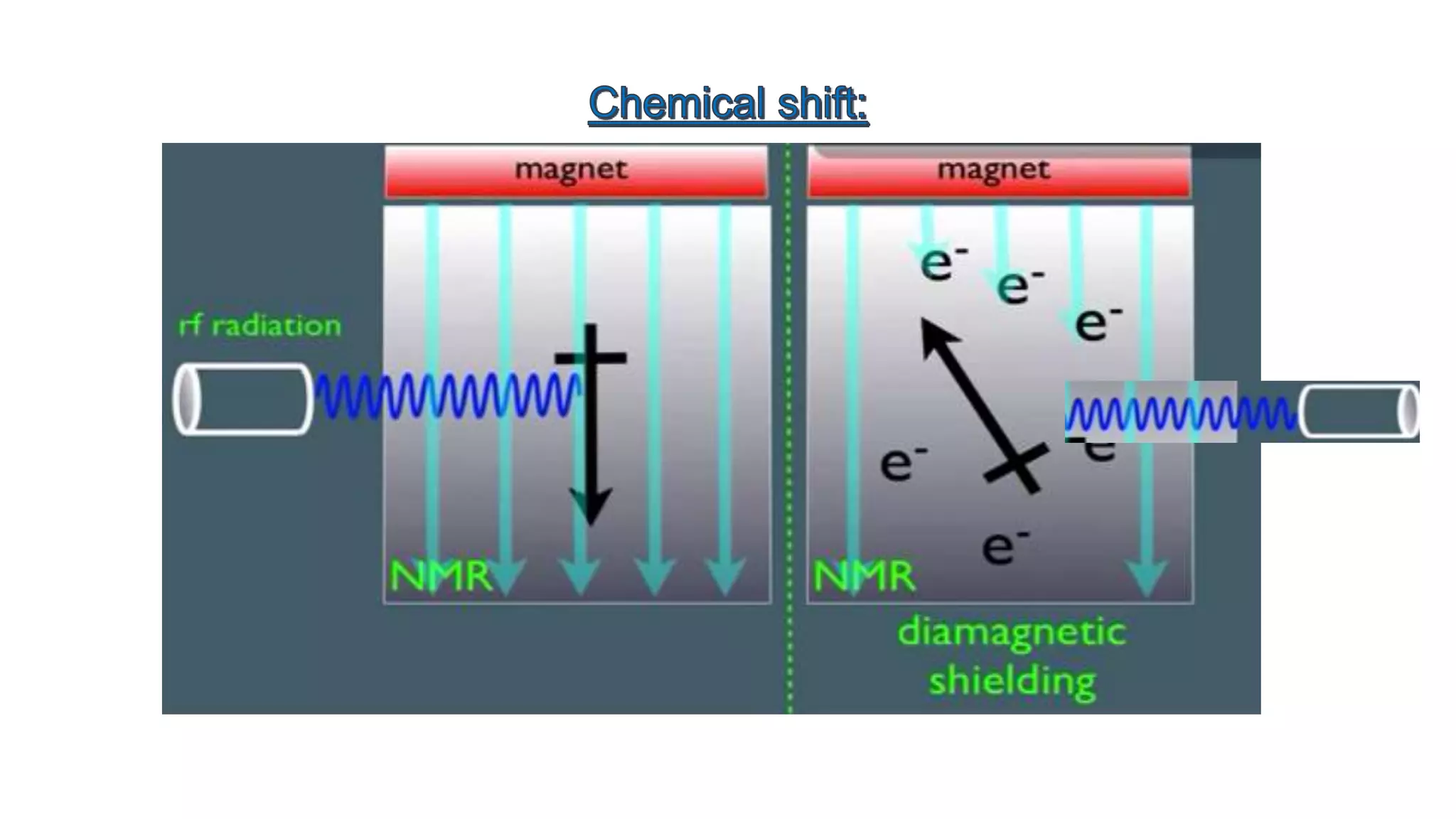
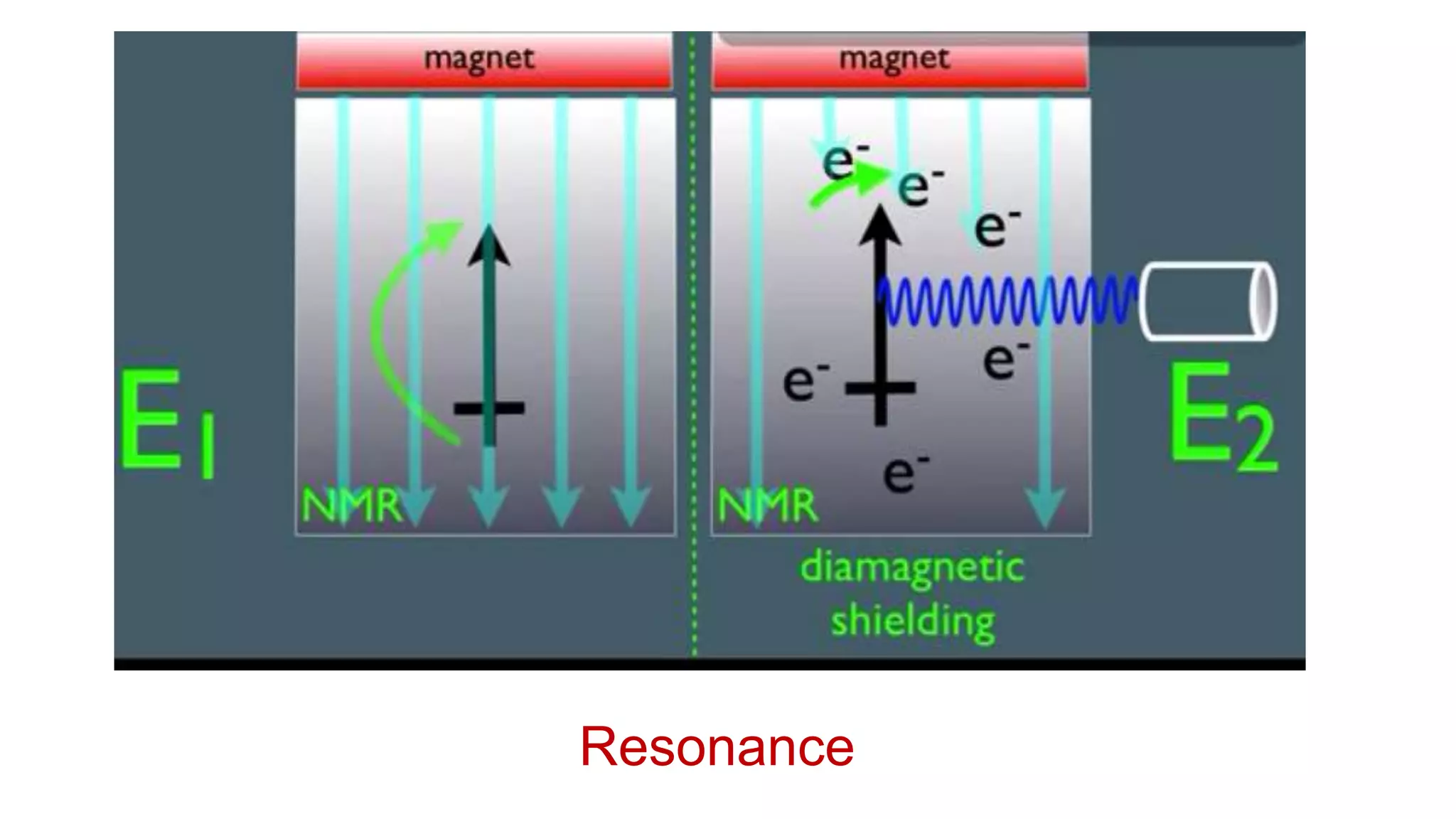
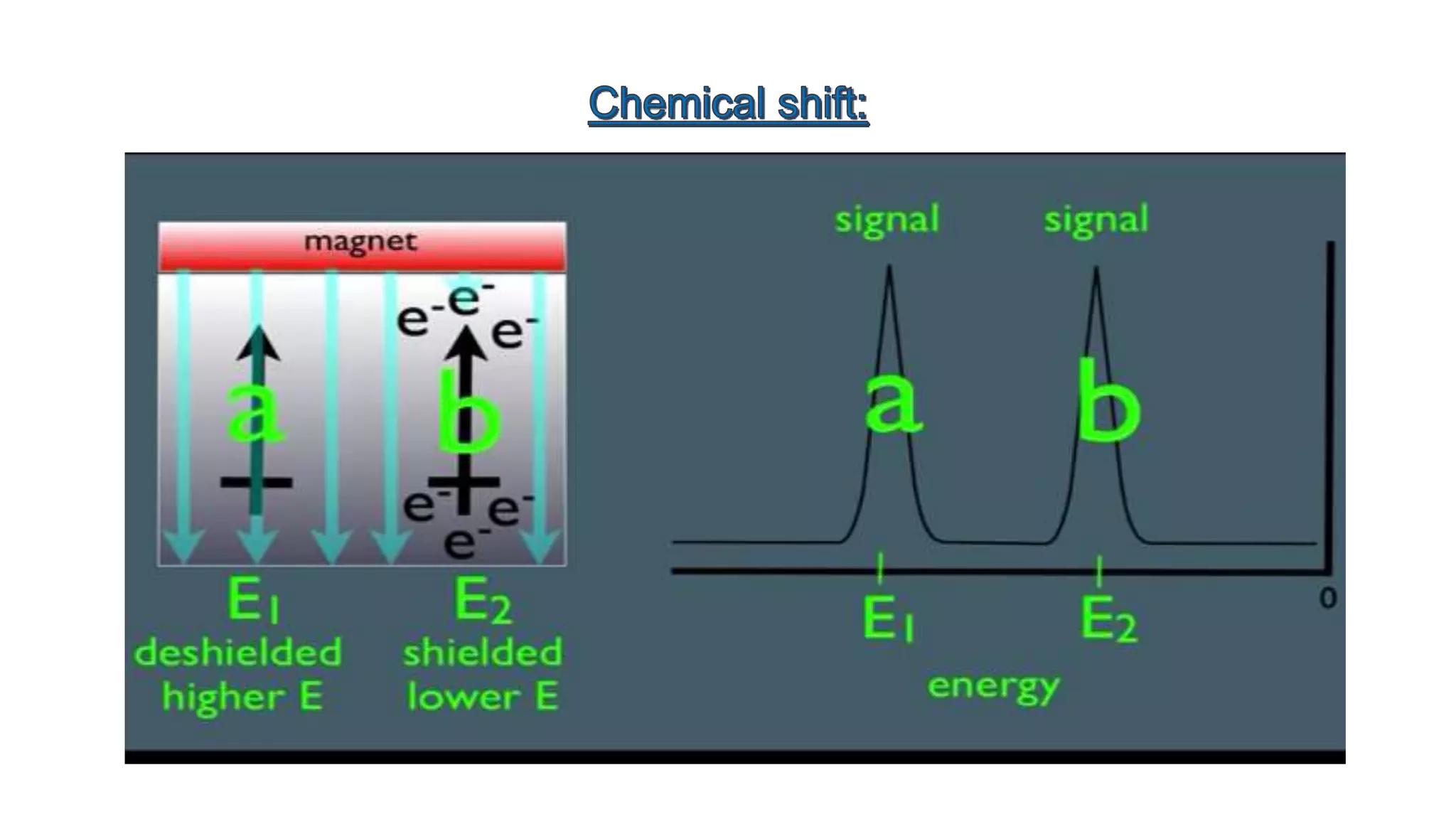
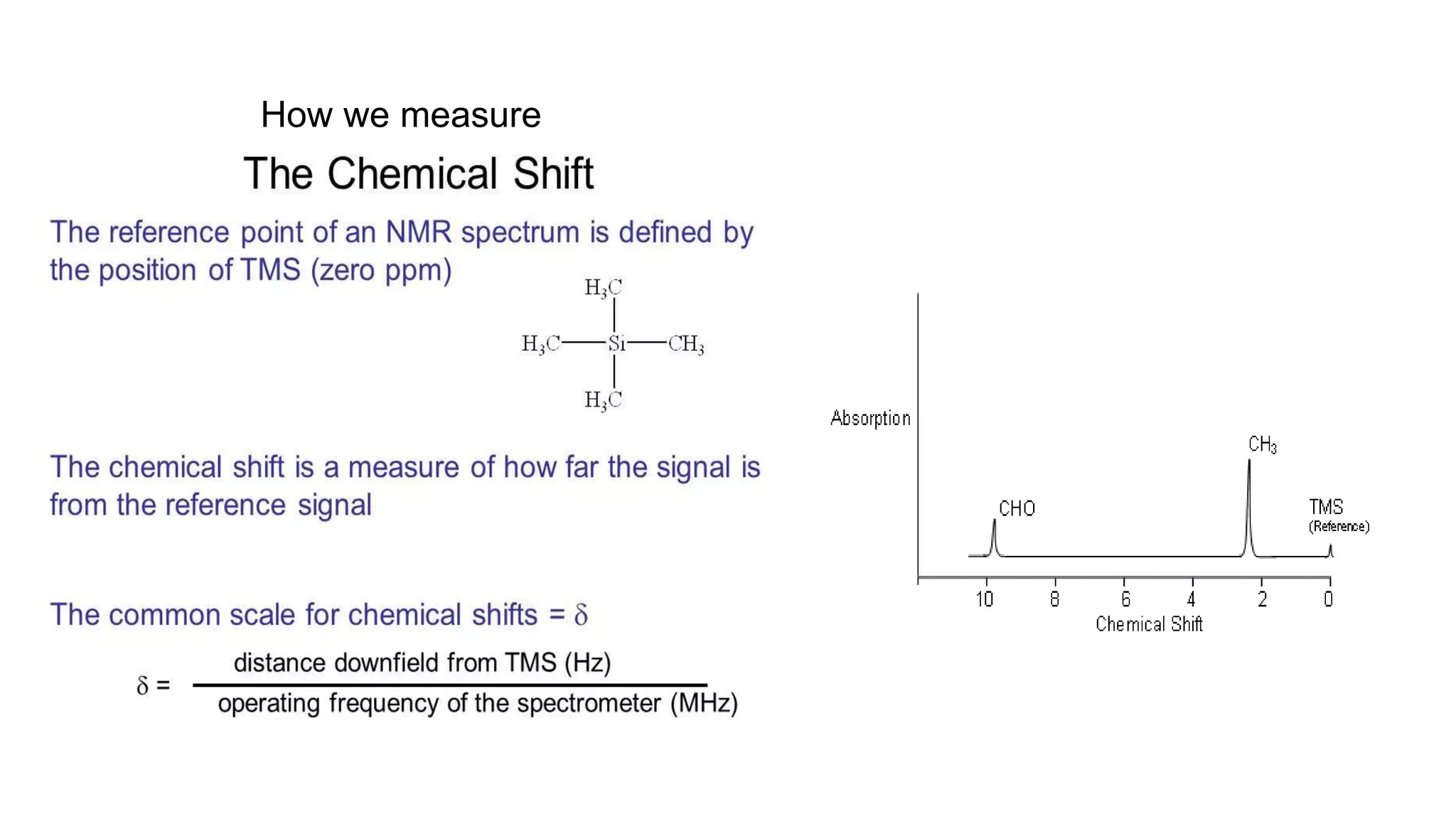
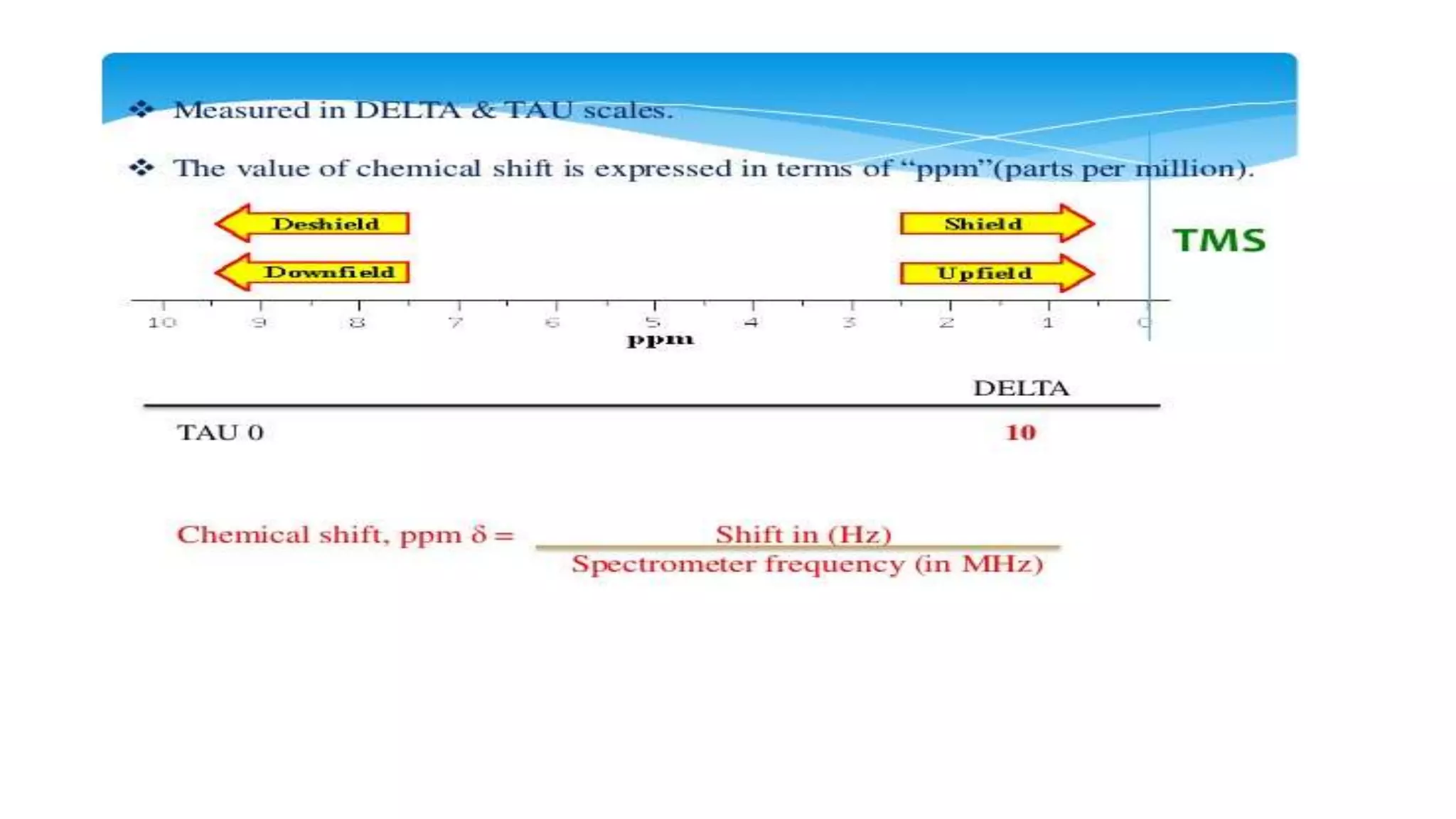
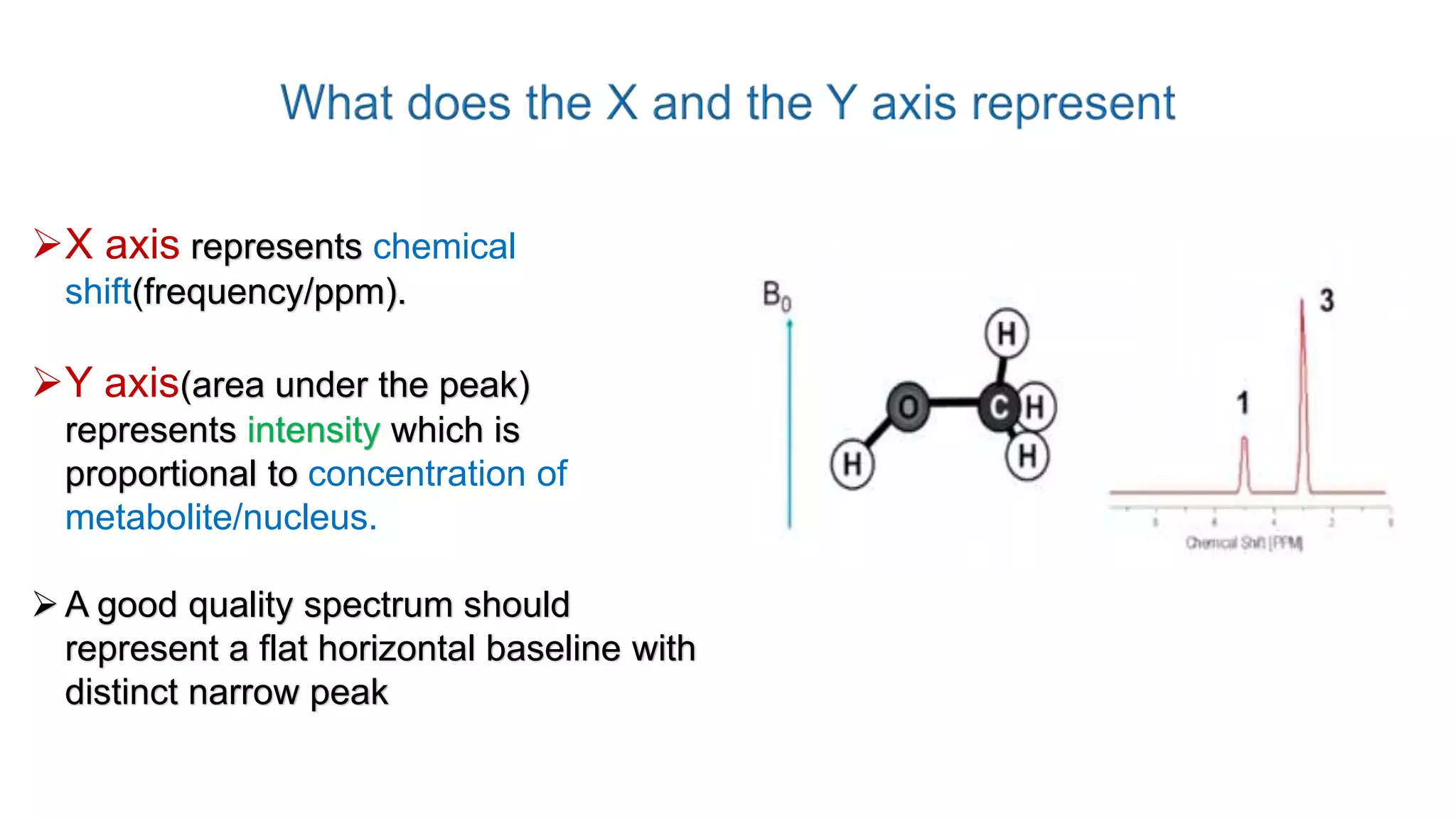
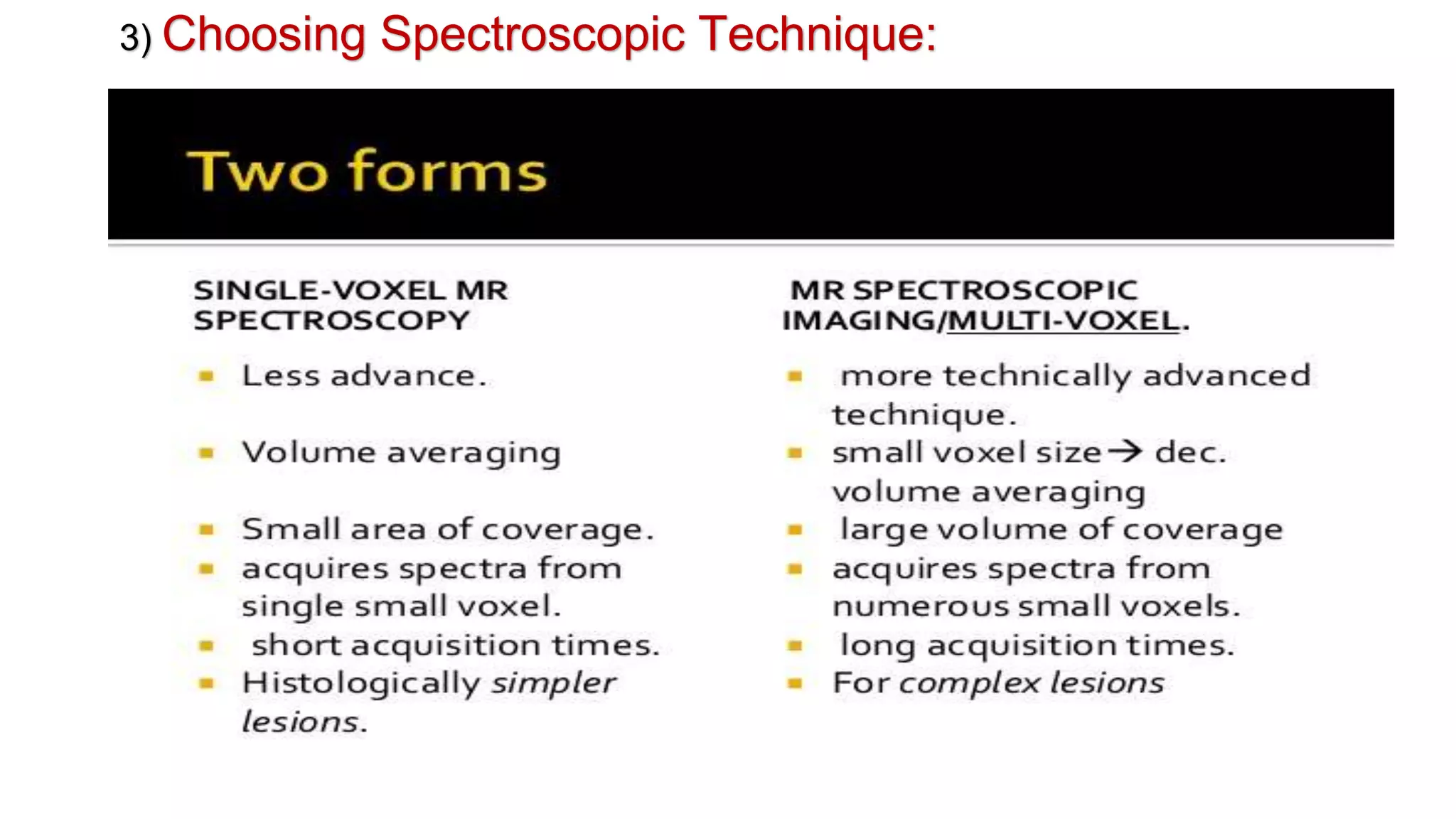
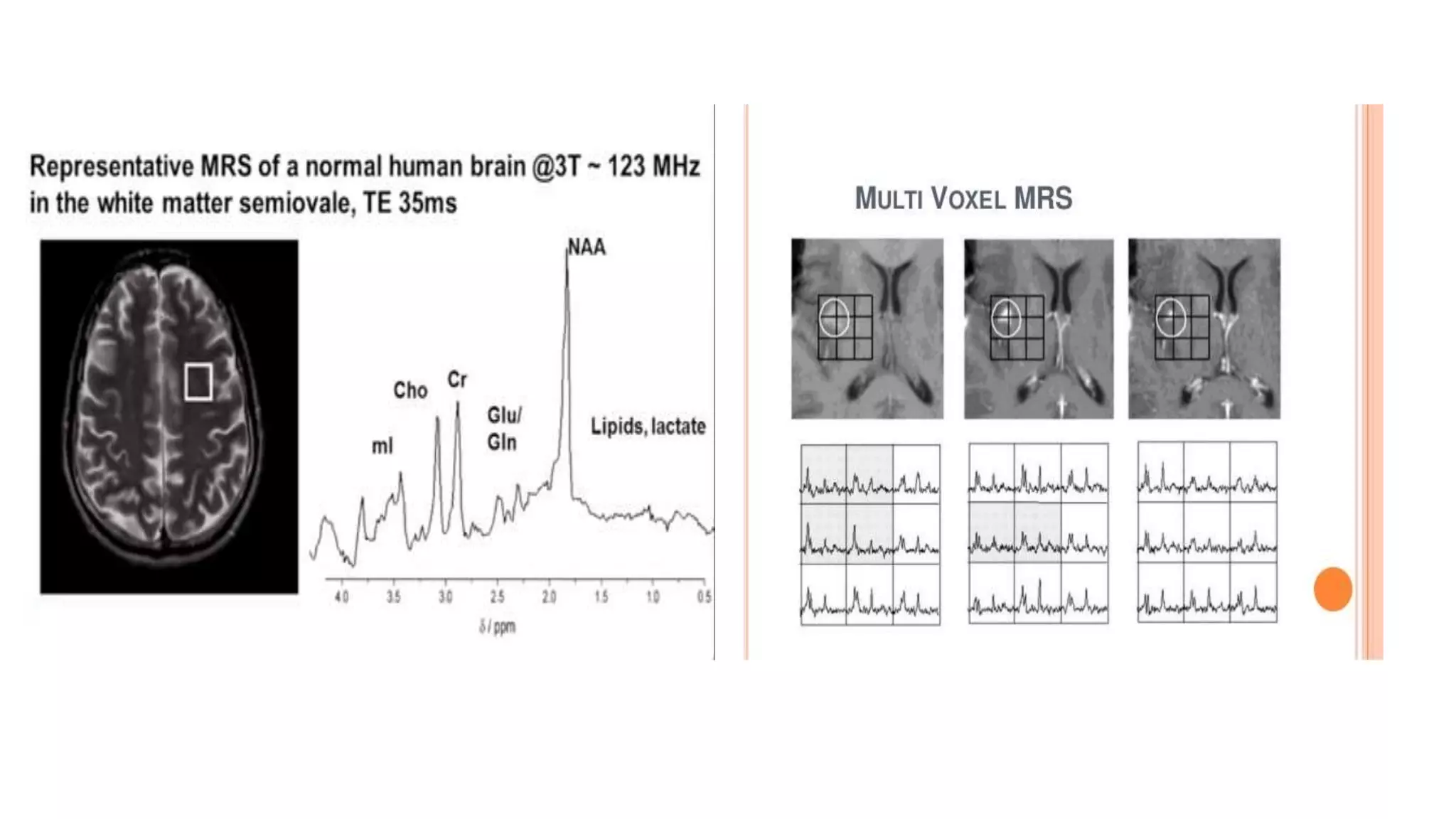
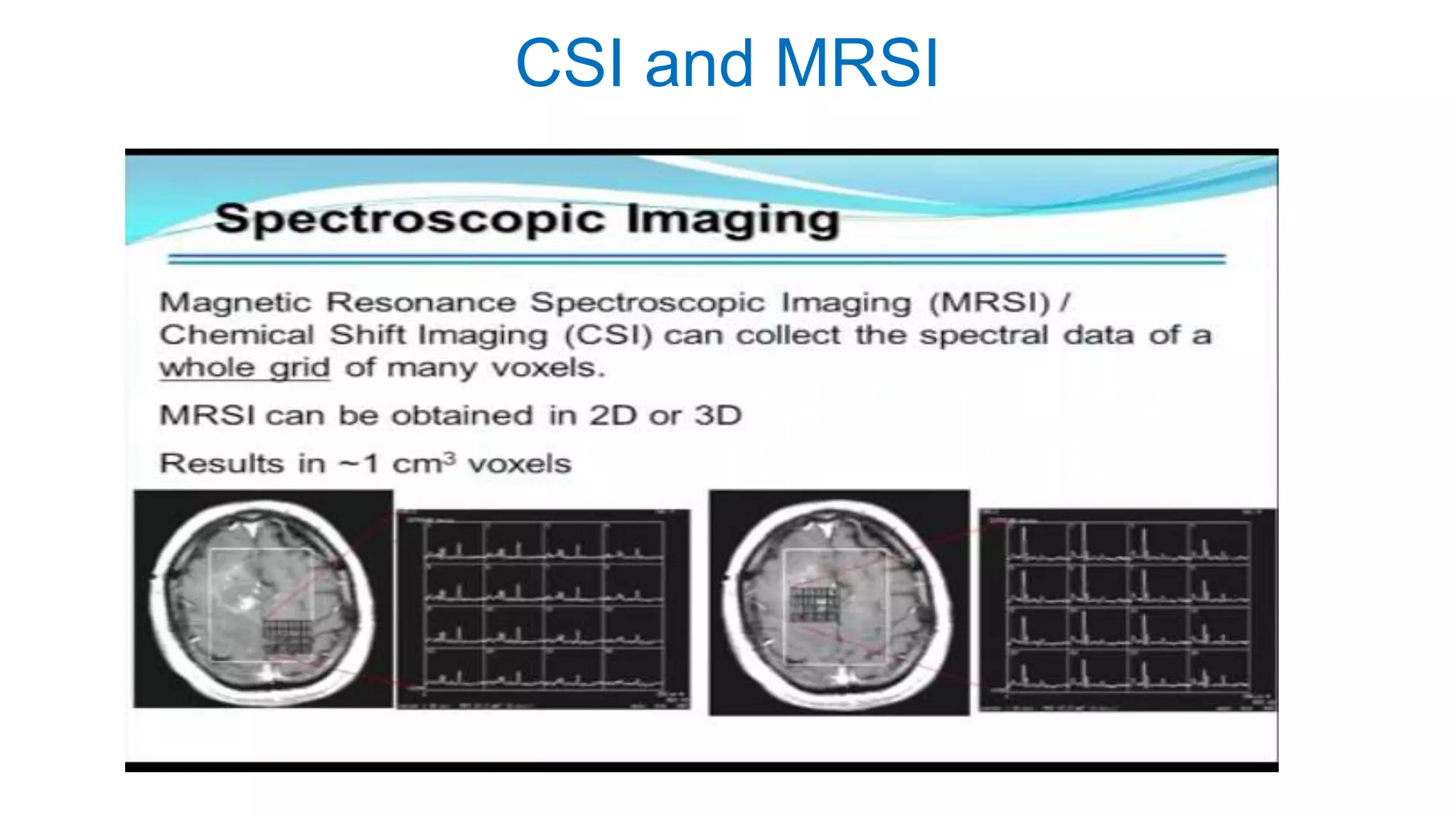
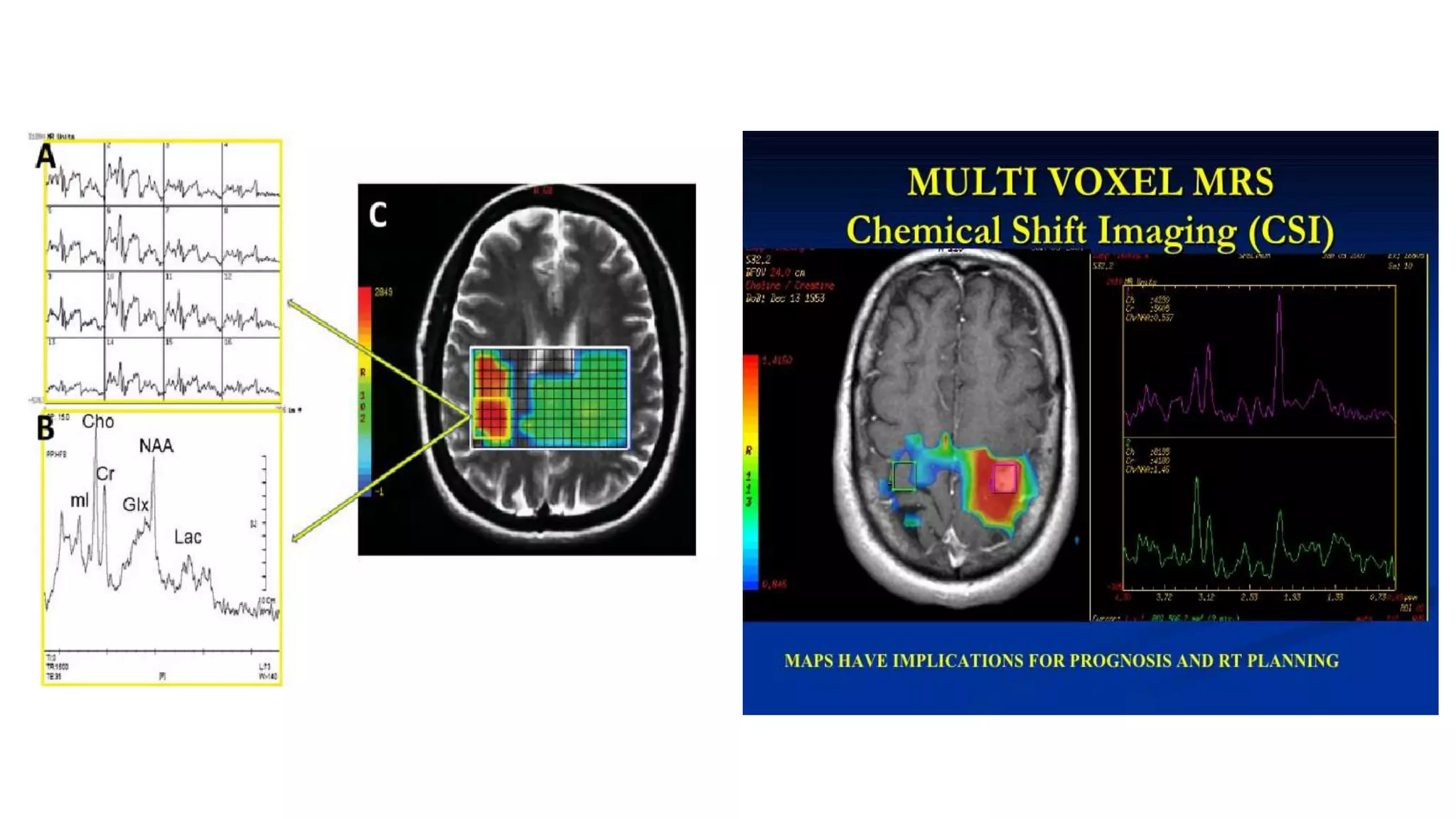
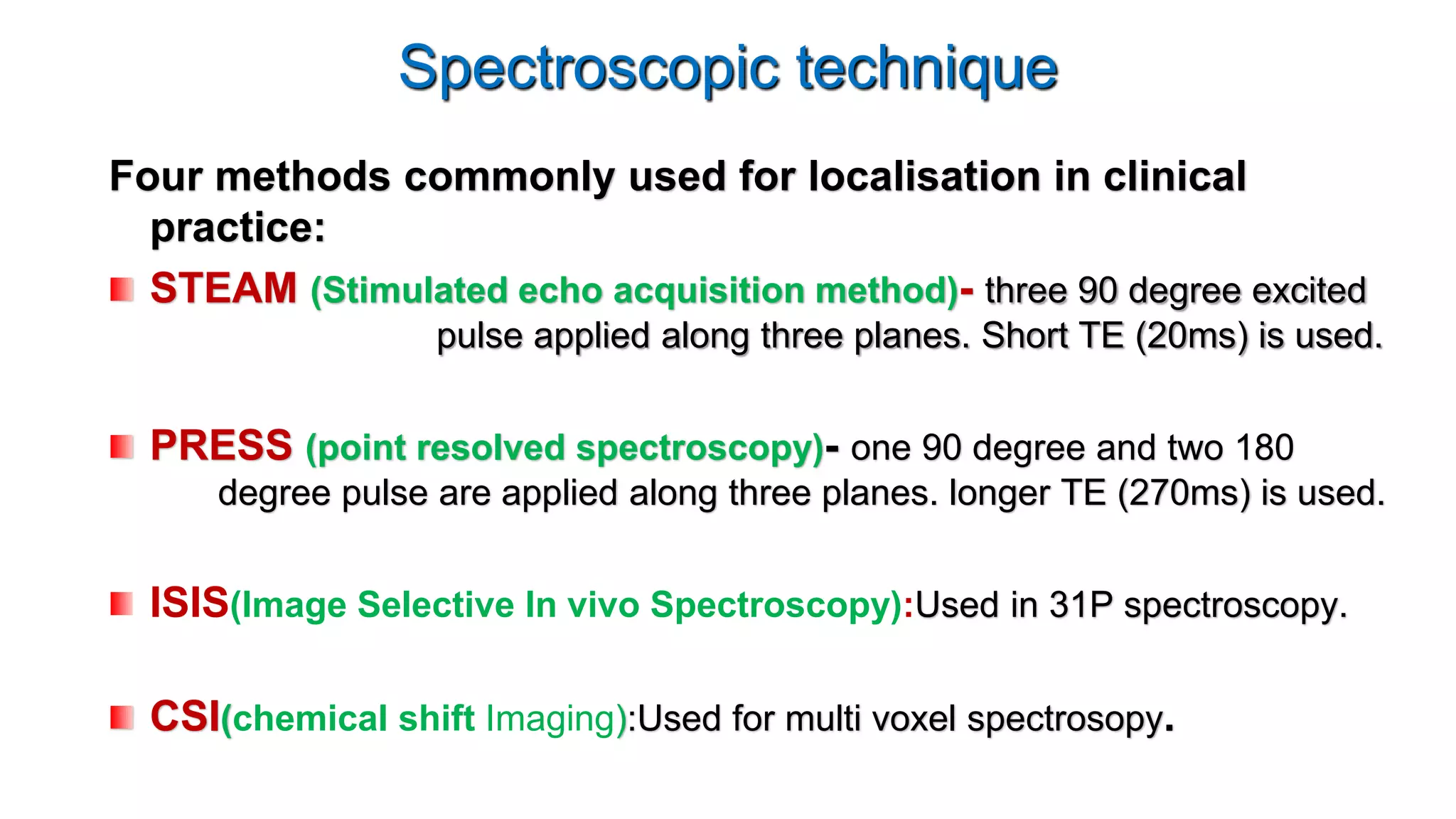
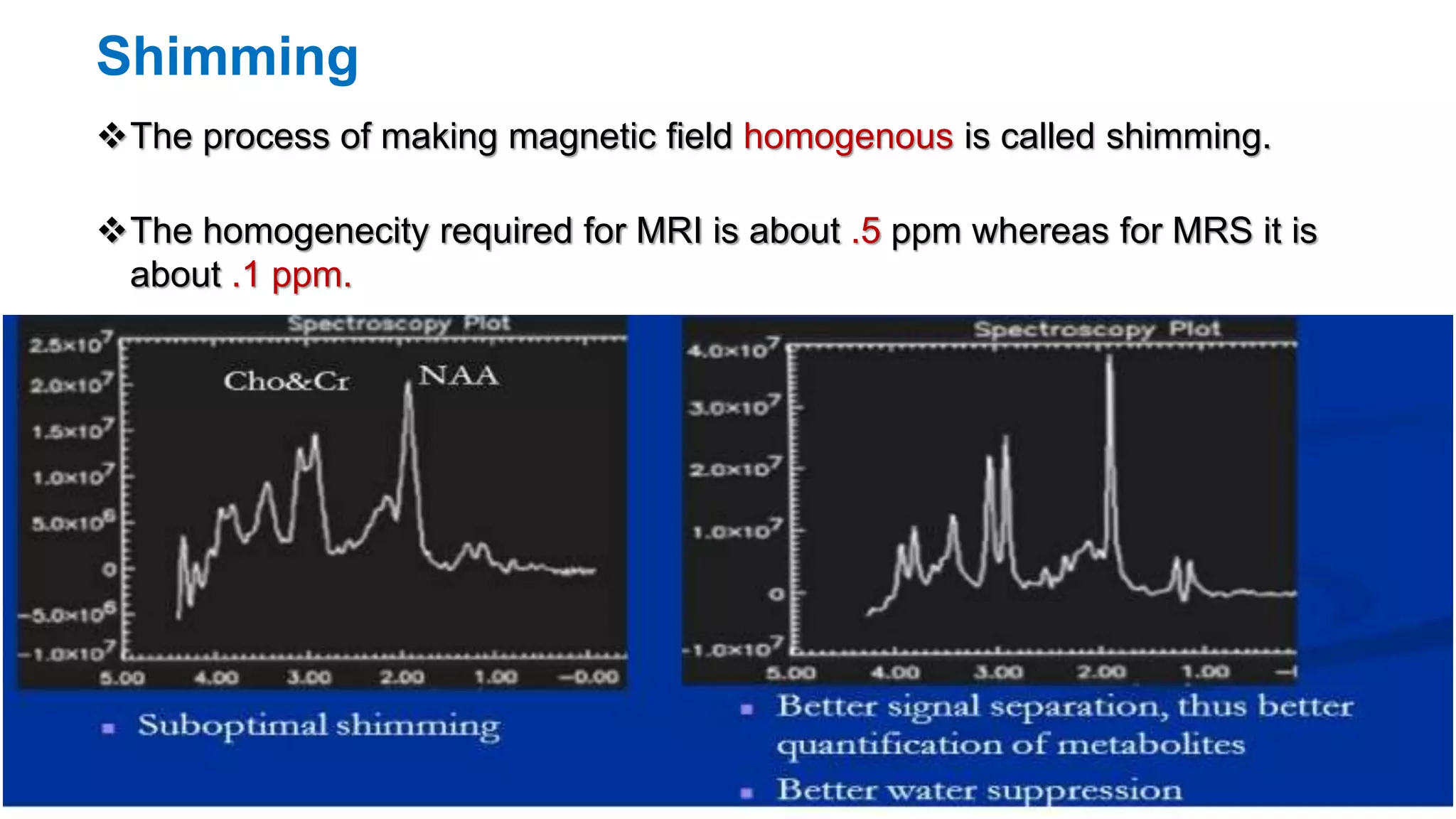
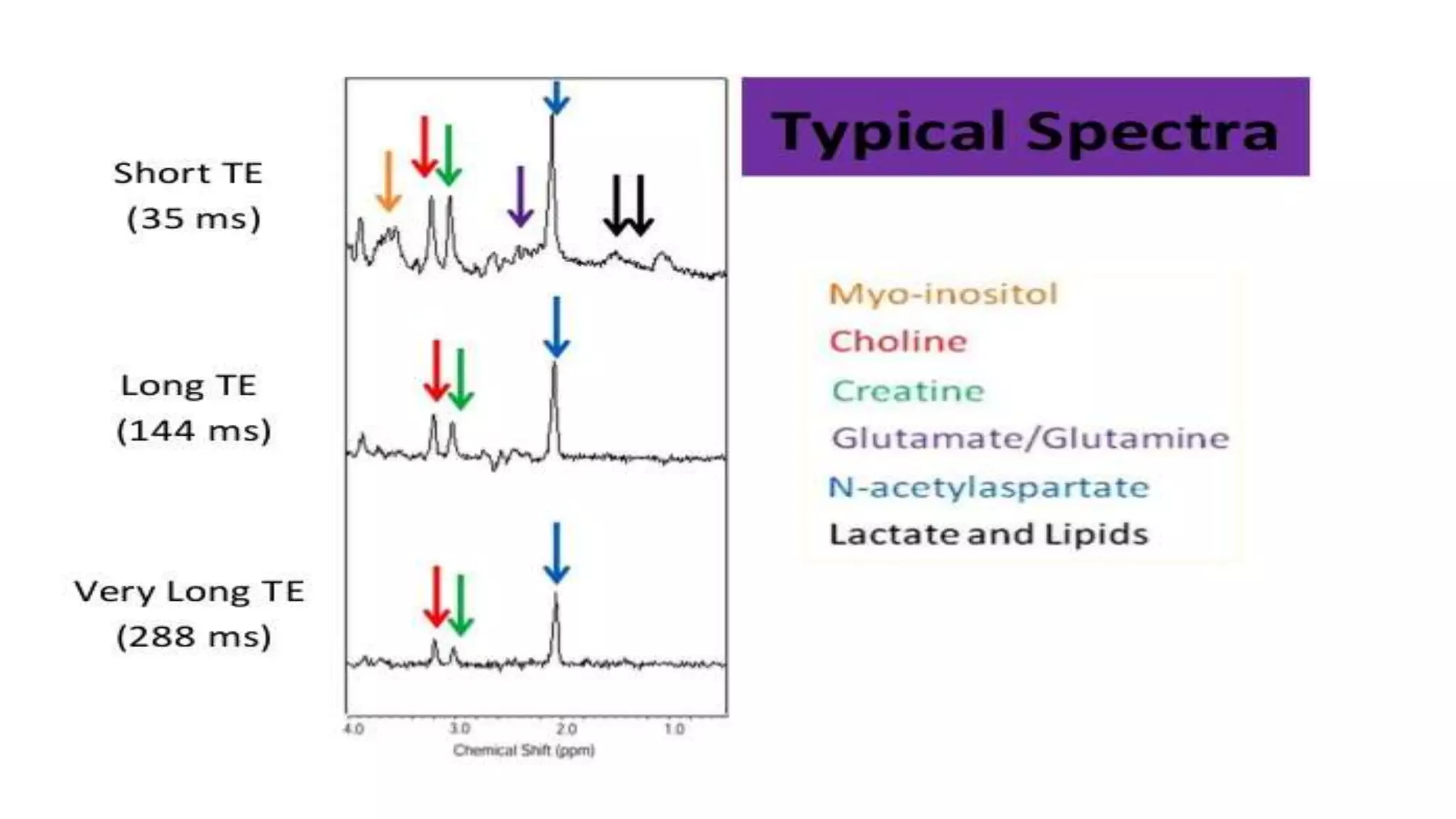
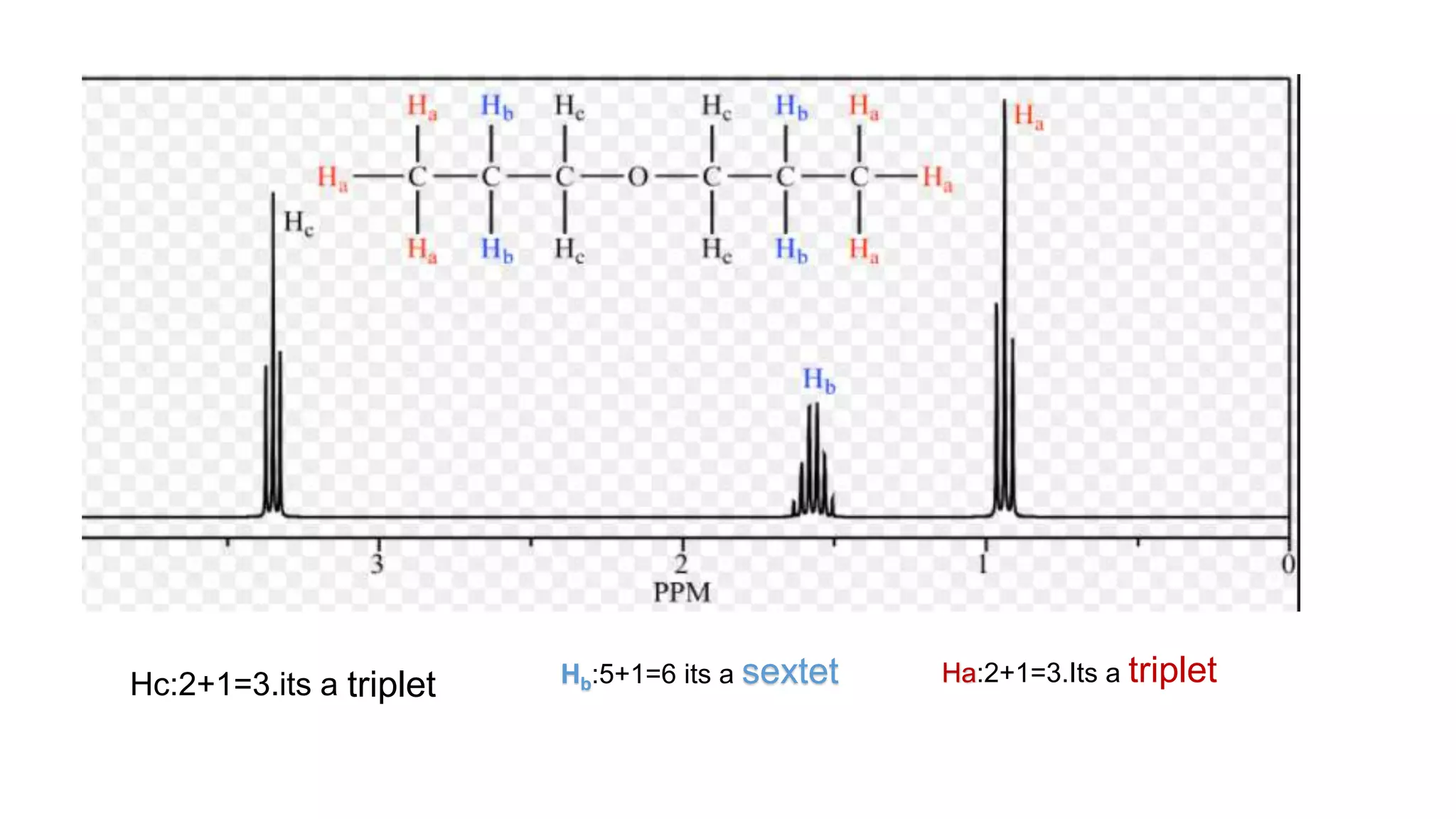
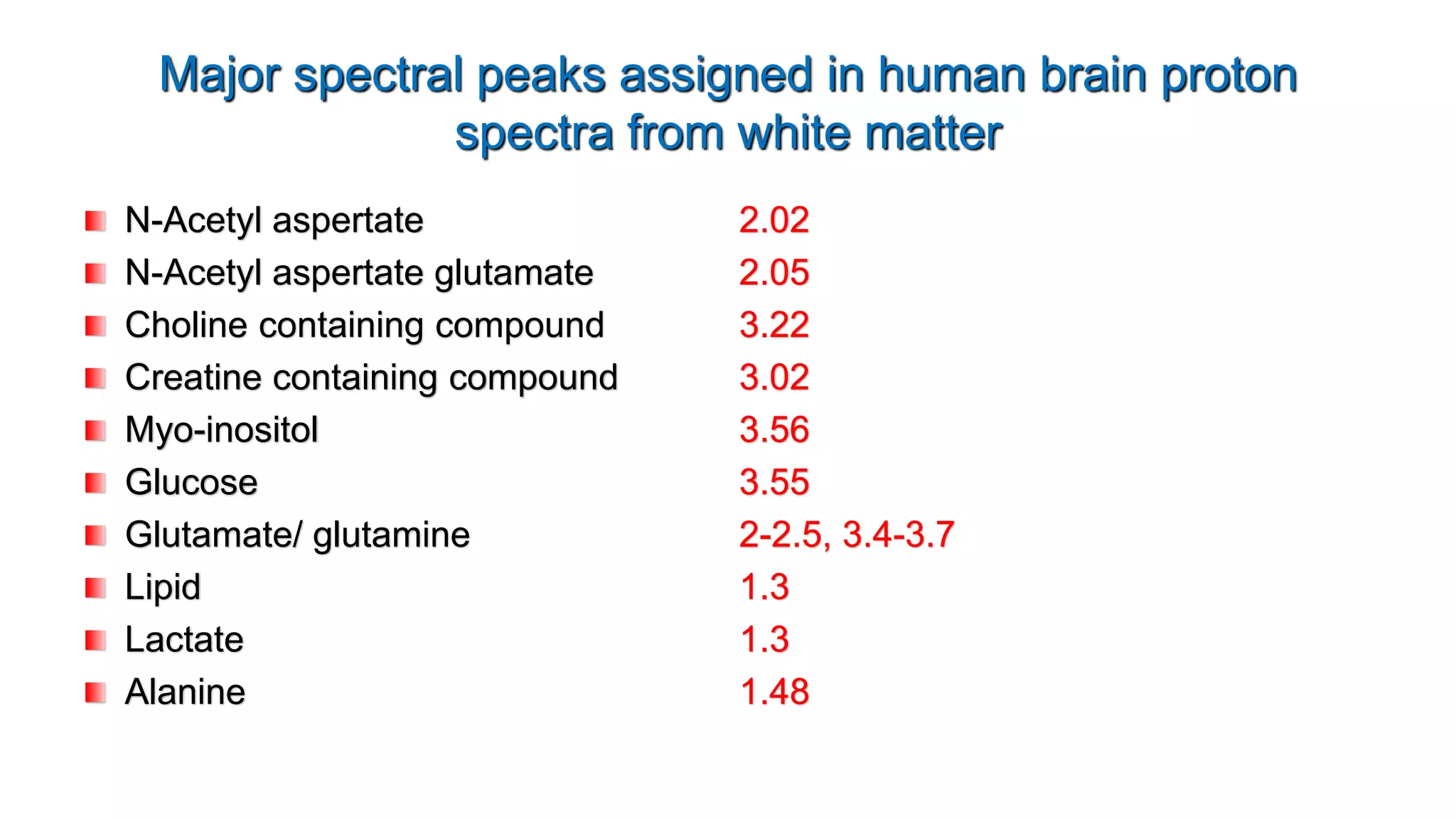
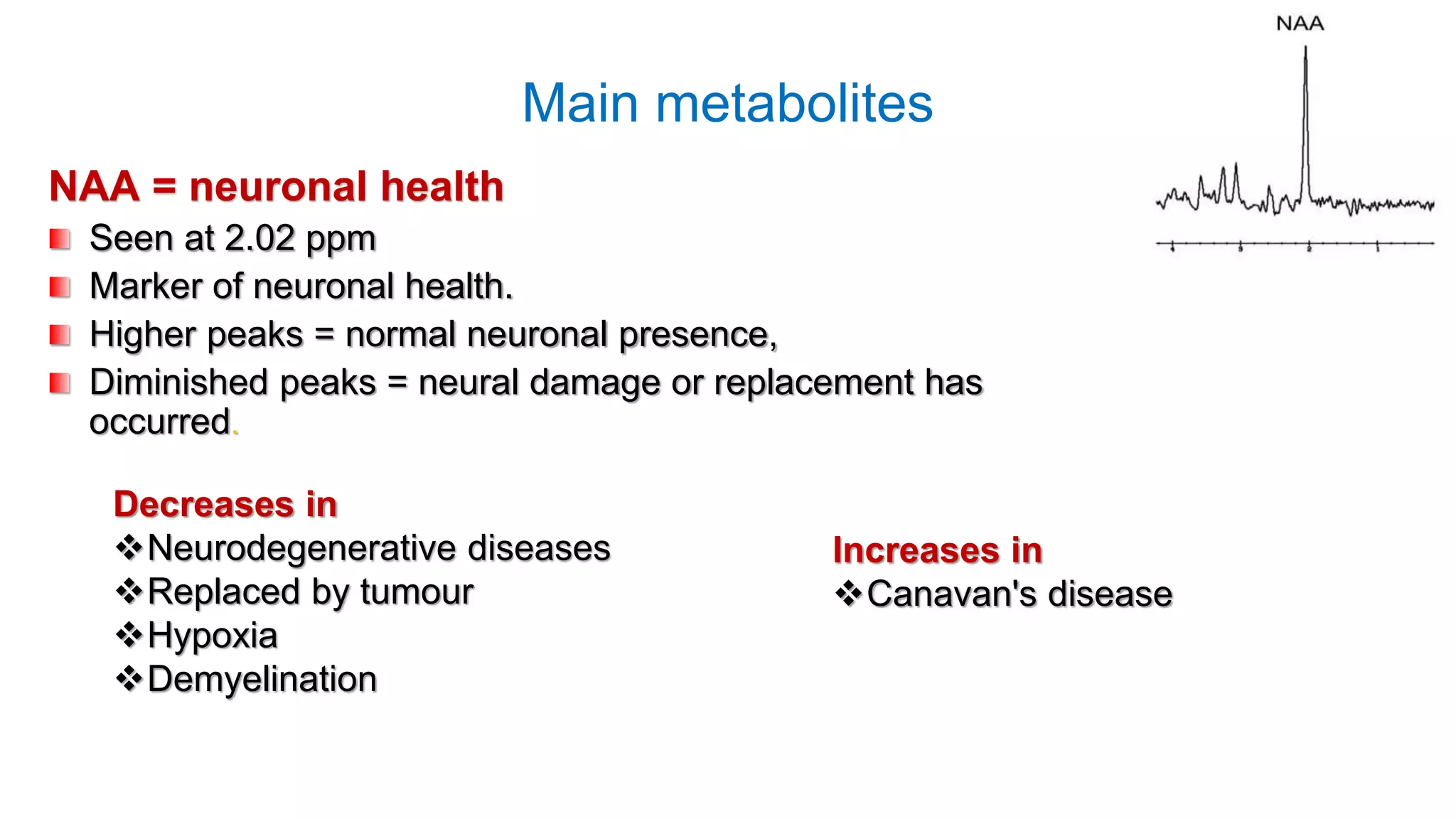
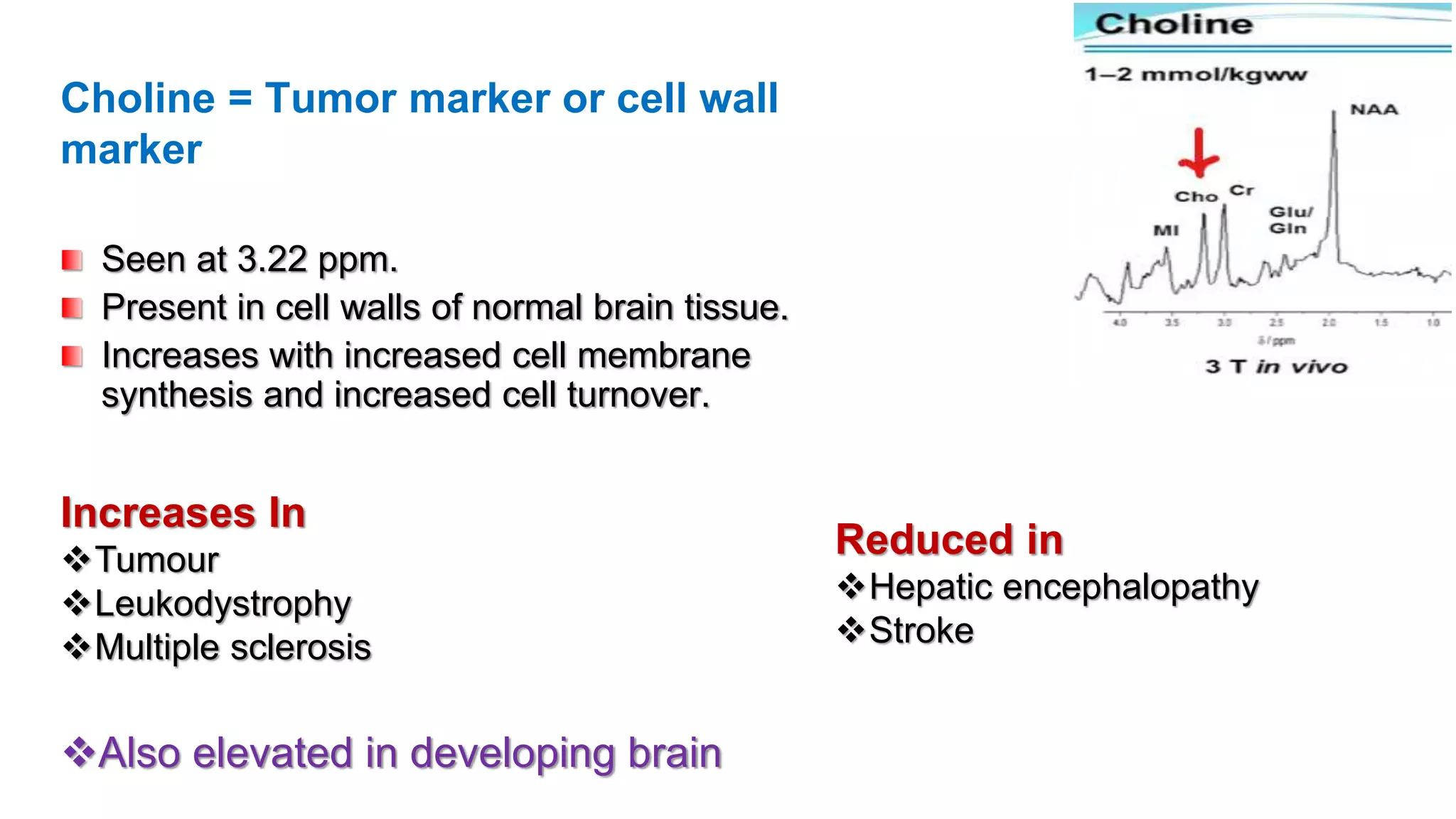
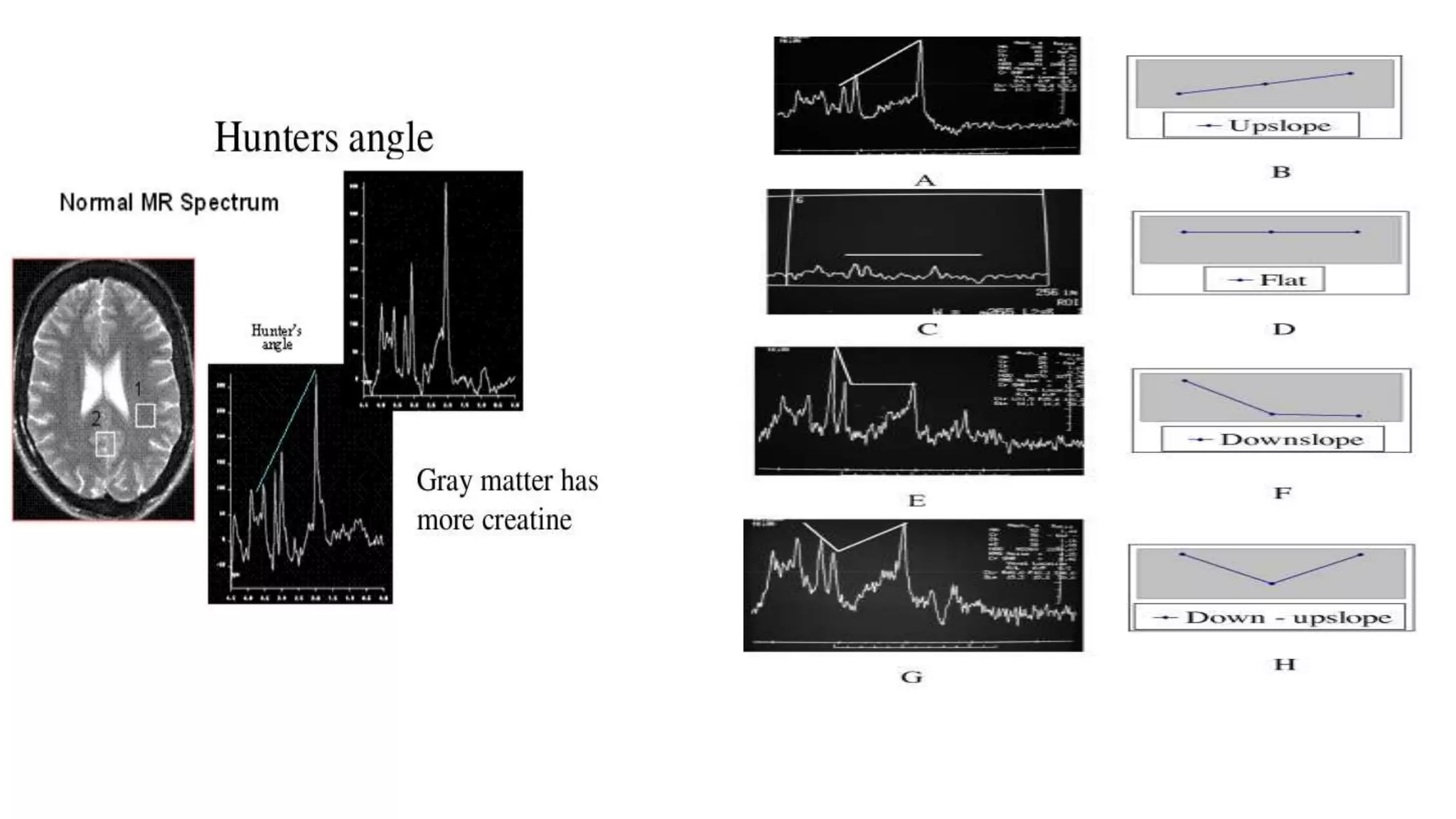
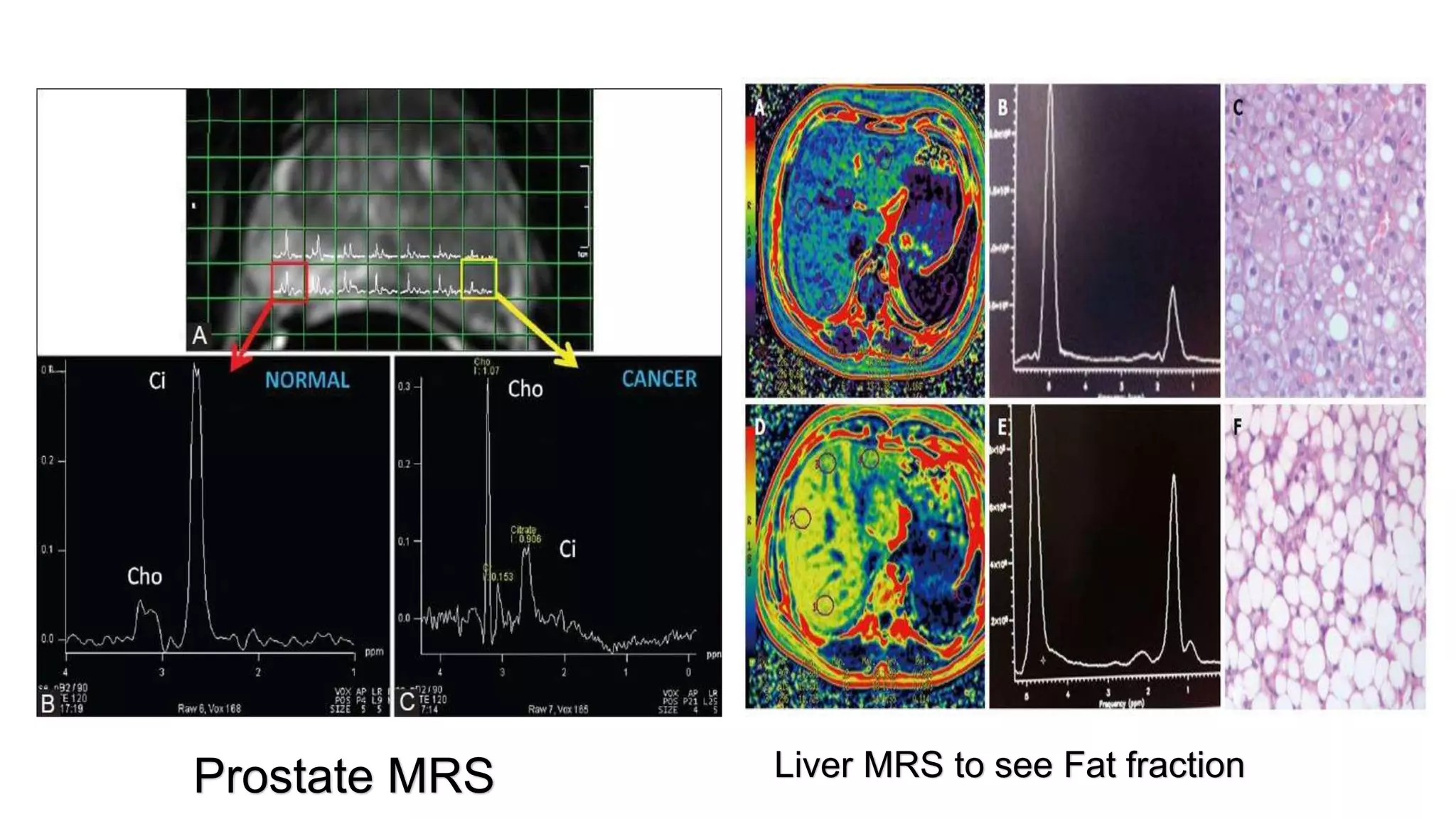
MRS provides quantitative measurements of metabolites in tissues by detecting their unique resonance frequencies, rather than producing an image based on proton signals. It can detect metabolites like NAA, choline, and creatine that provide information about neuronal health, cell turnover, and energy production. Obtaining a high quality MRS spectrum requires optimizing magnetic field homogeneity, suppressing the water signal, and using techniques like STEAM or PRESS for signal localization. Peaks are interpreted based on their chemical shift location and relative intensities. MRS is used clinically to evaluate conditions like tumors, infections, and neurodegenerative diseases.

















































![MRS_Presentation_BMRIT spectroscopy [1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/mrspresentationbmrit5thsem1-251126172259-1b1e9db3-thumbnail.jpg?width=640&height=640&fit=bounds)




















