
Downloaded 61 times

![Peritoneal fluid (ascitic fluid) analysis
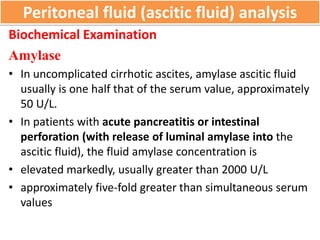
Biochemical Examination
LDH
• Normally, LDH molecule is too large to enter the ascitic
fluid readily from blood.
• [LDH] in ascitic fluid is usually less than one half of the
serum level (uncomplicated cirrhotic ascites)
• In SBP, ascitic fluid LDH level rises because of the release
of LDH from neutrophils.
• In secondary peritonitis, LDH ascitic fluid > LDH serum ,
higher than those in SBP](https://image.slidesharecdn.com/asciticfluidexamination-200420102558/85/Ascitic-fluid-examination-13-320.jpg)


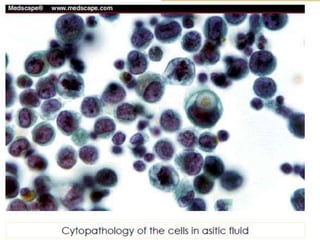
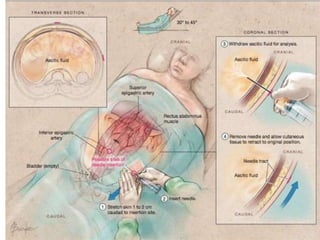
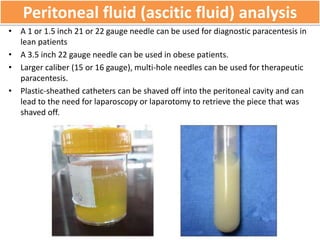
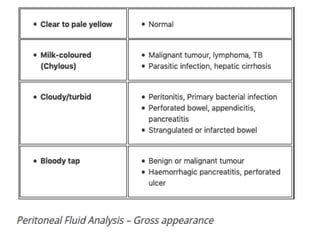
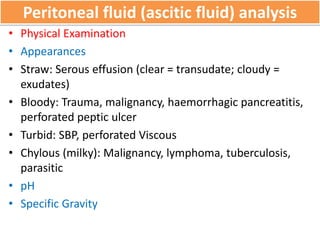
The document discusses the analysis of ascitic fluid, which is abnormal fluid accumulation in the abdomen. Key points: 1. Ascitic fluid analysis involves examining the fluid's physical appearance, biochemical properties, microscopic cells, culture results, and cytology/molecular testing to determine the cause of fluid buildup and diagnose conditions like cancer, infection, or liver disease. 2. Transudative ascites has a low protein level (<30g/L) and is caused by systemic diseases like liver cirrhosis, while exudative ascites has a high protein level (>30g/L) and results from local abdominal diseases. 3. The serum-ascites albumin gradient measured the fluid protein




![serous fluid Dr shweta [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/serousfluiddrshwetaautosaved-221213040107-a9b2a766-thumbnail.jpg?width=640&height=640&fit=bounds)






























































