Downloaded 2,981 times






















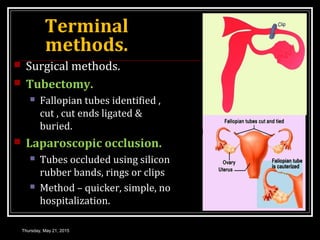




















This document discusses various contraceptive methods for both males and females. It begins by outlining the objectives of contraception and characteristics of an ideal contraceptive. It then describes spacing and terminal contraceptive methods for females, including barrier methods like diaphragms, chemical methods like oral contraceptive pills and injectables, and intrauterine devices. Similar spacing and terminal methods are covered for males, such as condoms, withdrawal, and hormonal treatments. The aims, mechanisms of action, advantages and disadvantages are provided for each method.