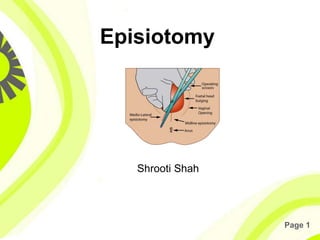

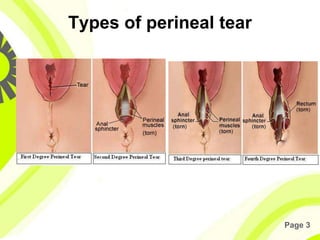











Episiotomy is a surgical incision in the perineum and vaginal wall during labor, aimed at facilitating delivery and minimizing tears. It has specific indications such as rigid perineum and certain delivery methods, and various types include median and medio-lateral, each with pros and cons. The procedure involves careful preparation, execution, and repair, with potential complications such as infection and extensions to the rectum.