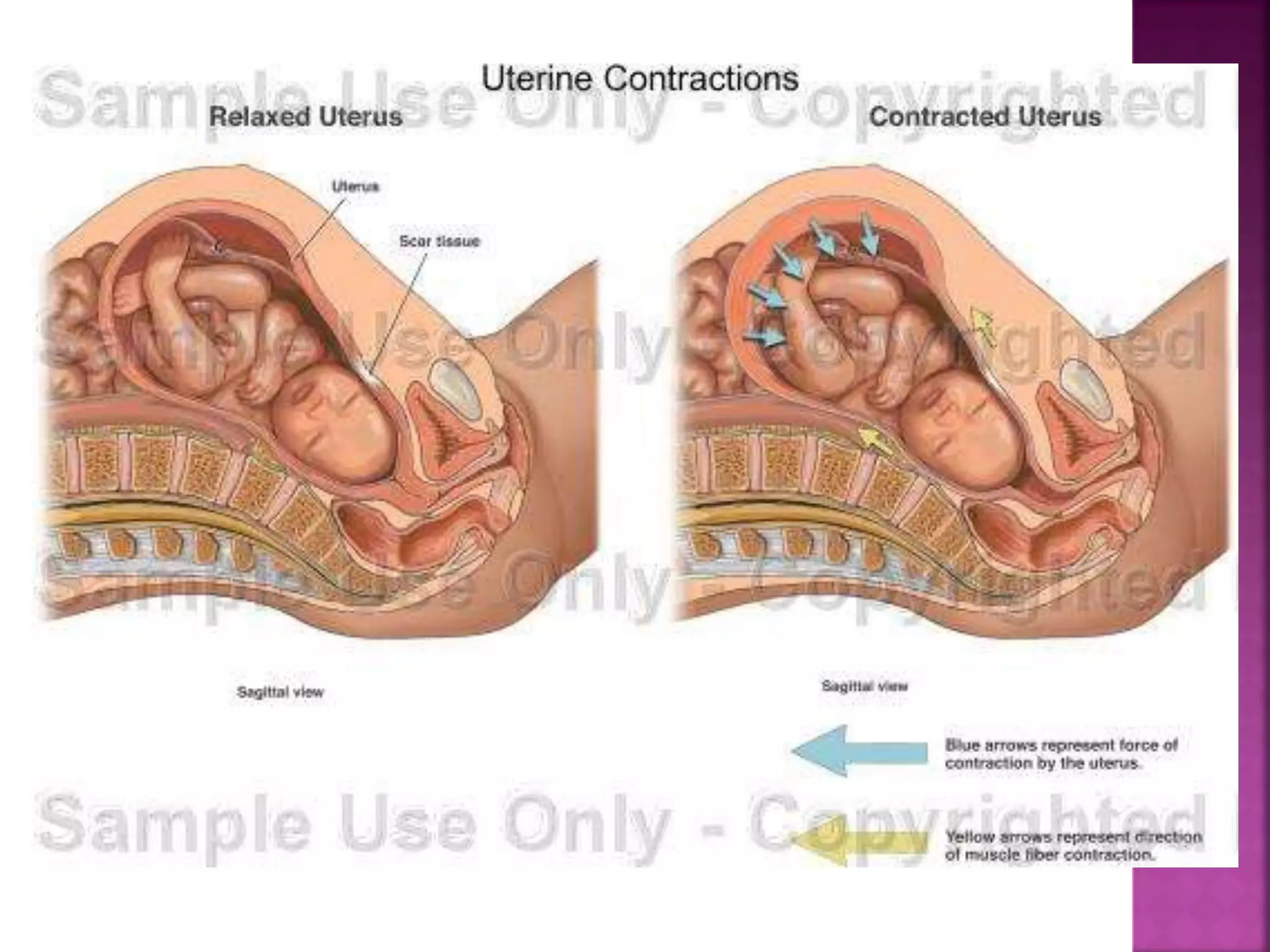
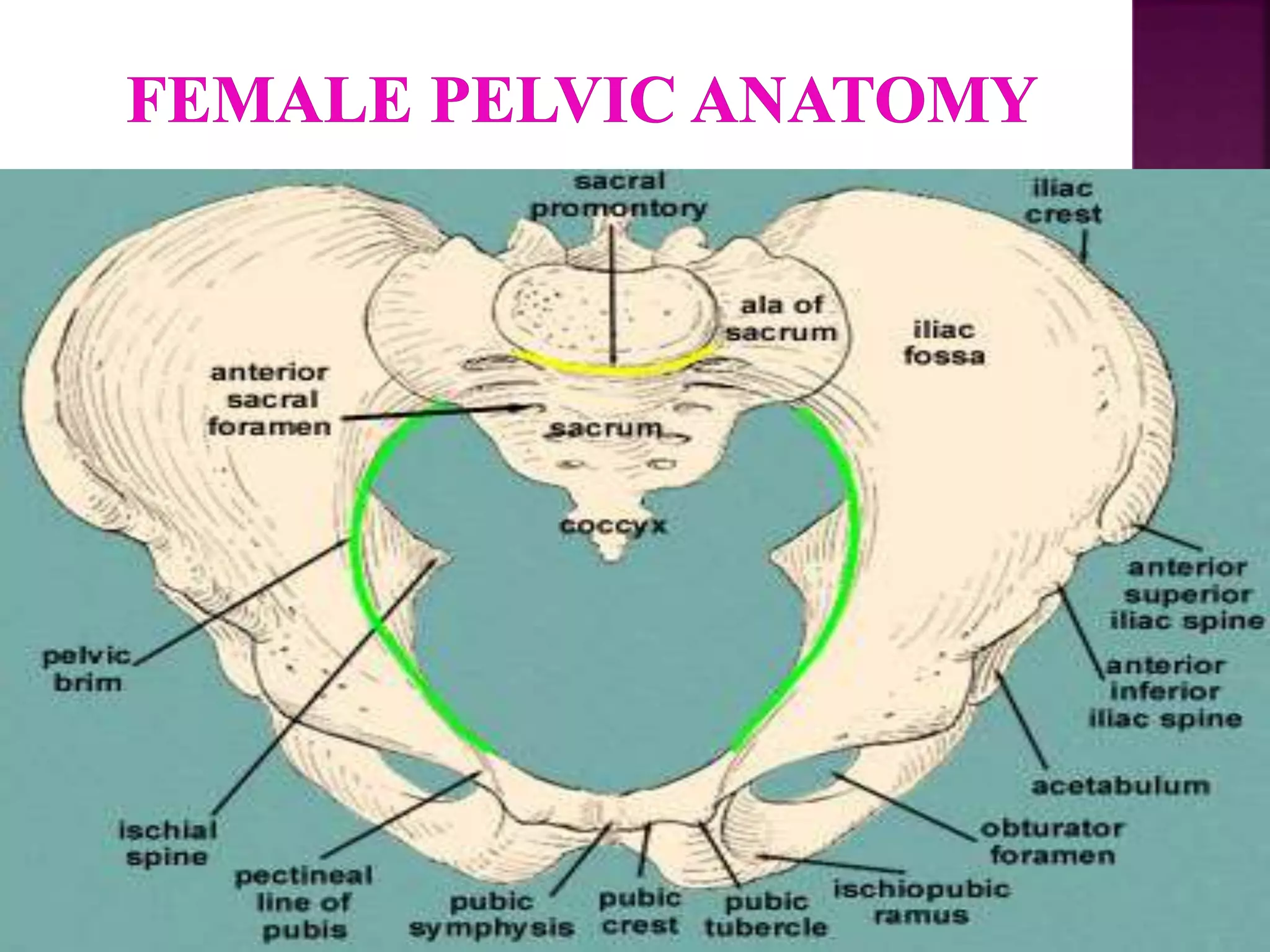
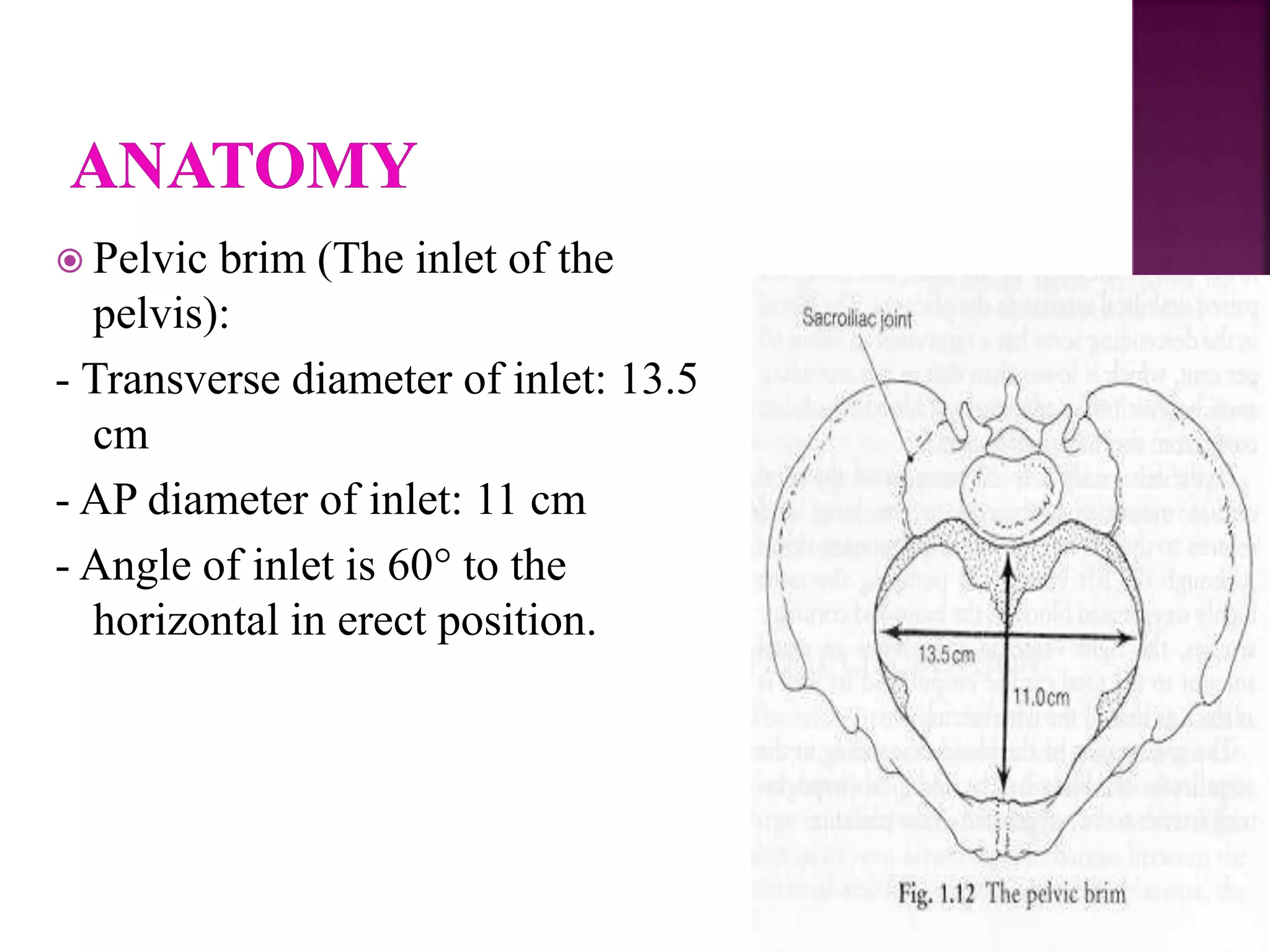
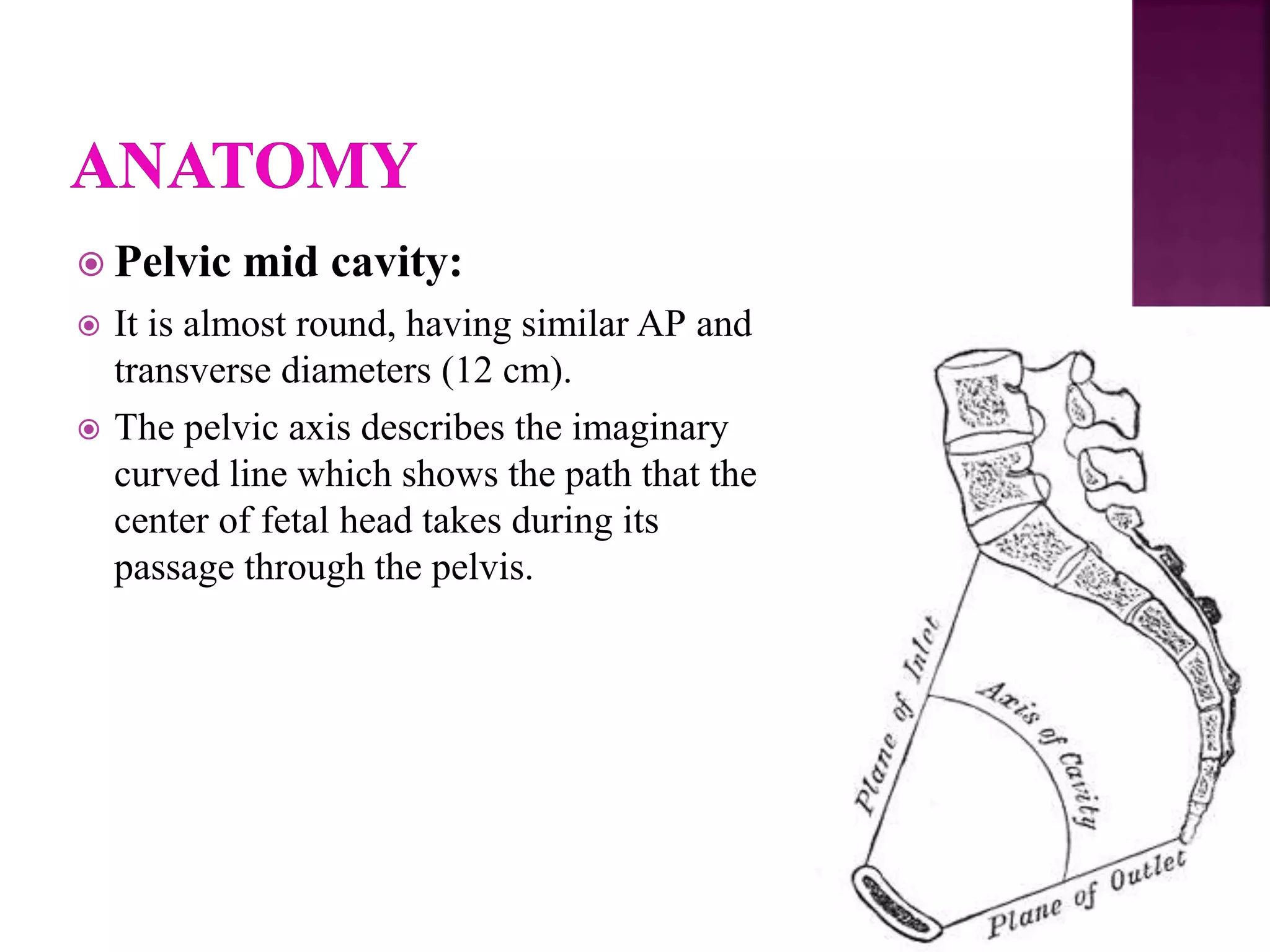
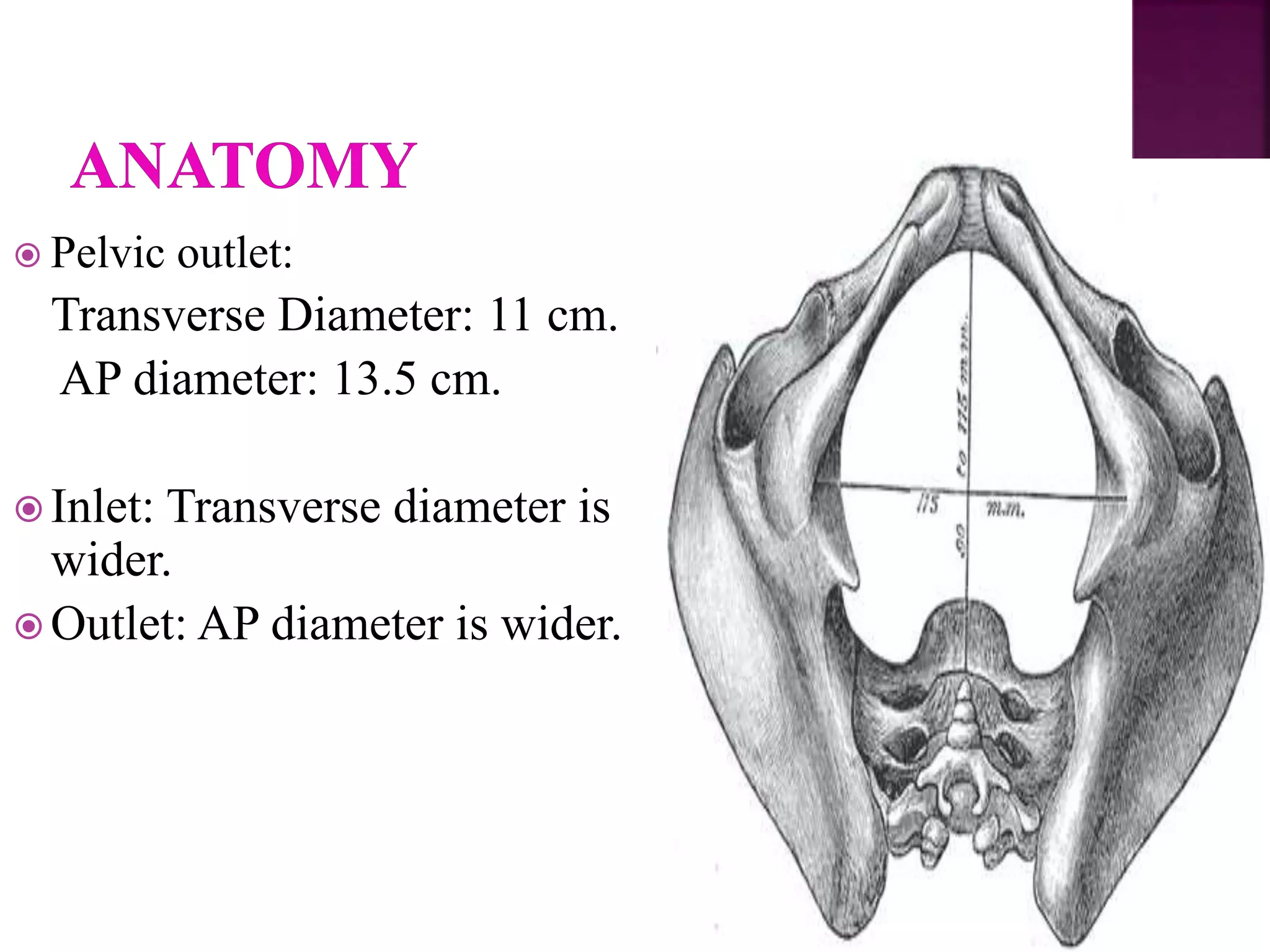
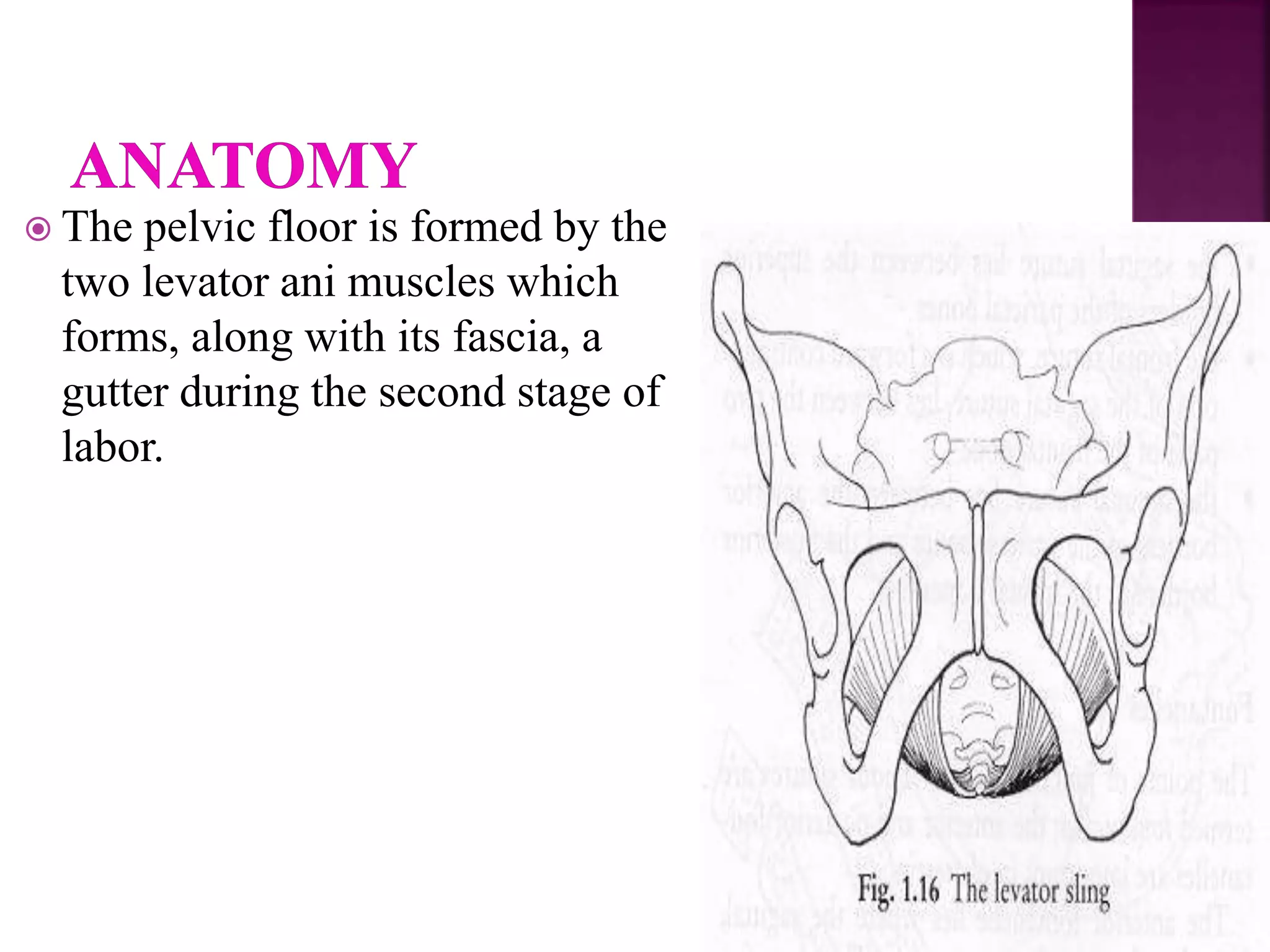
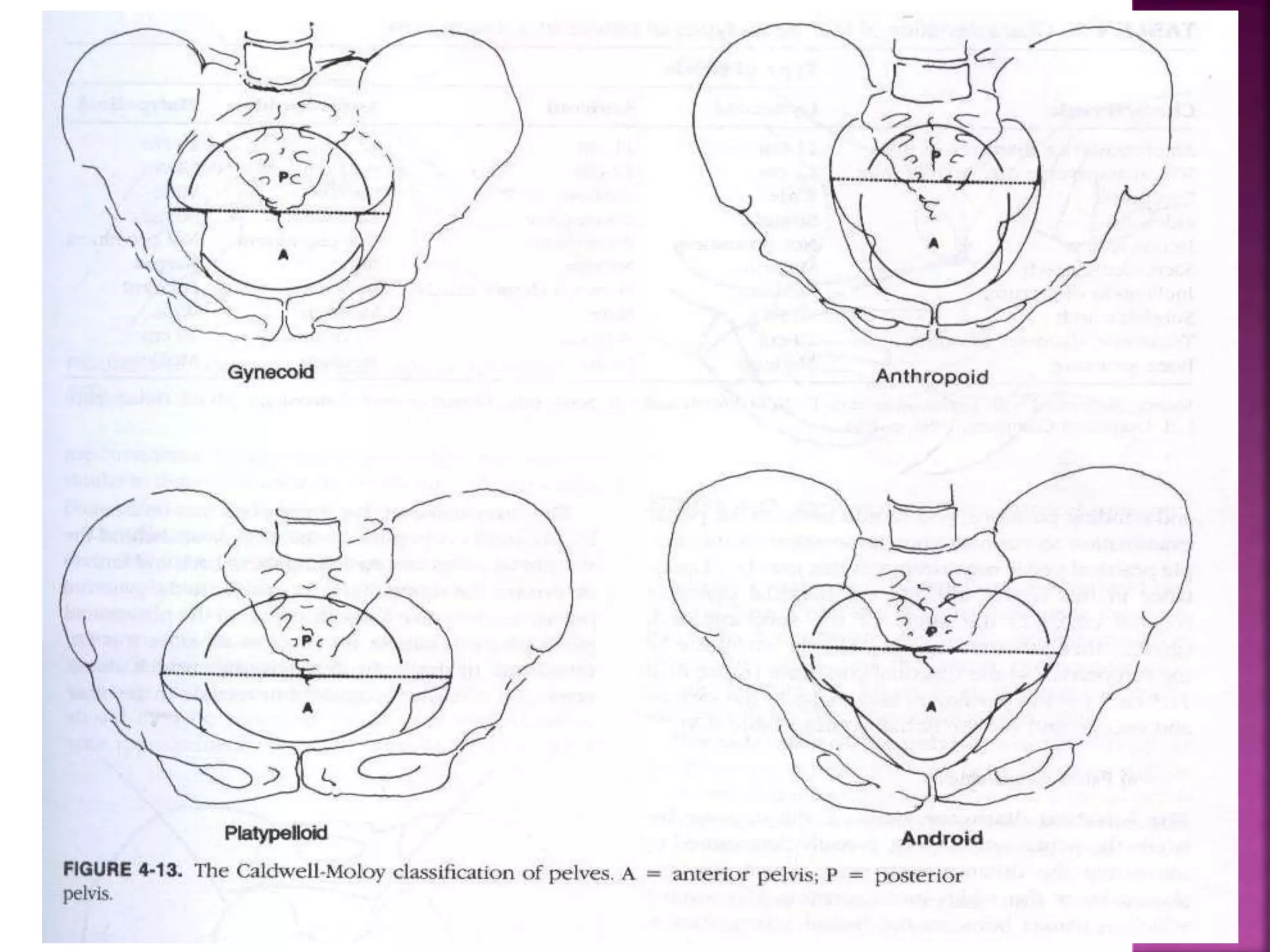
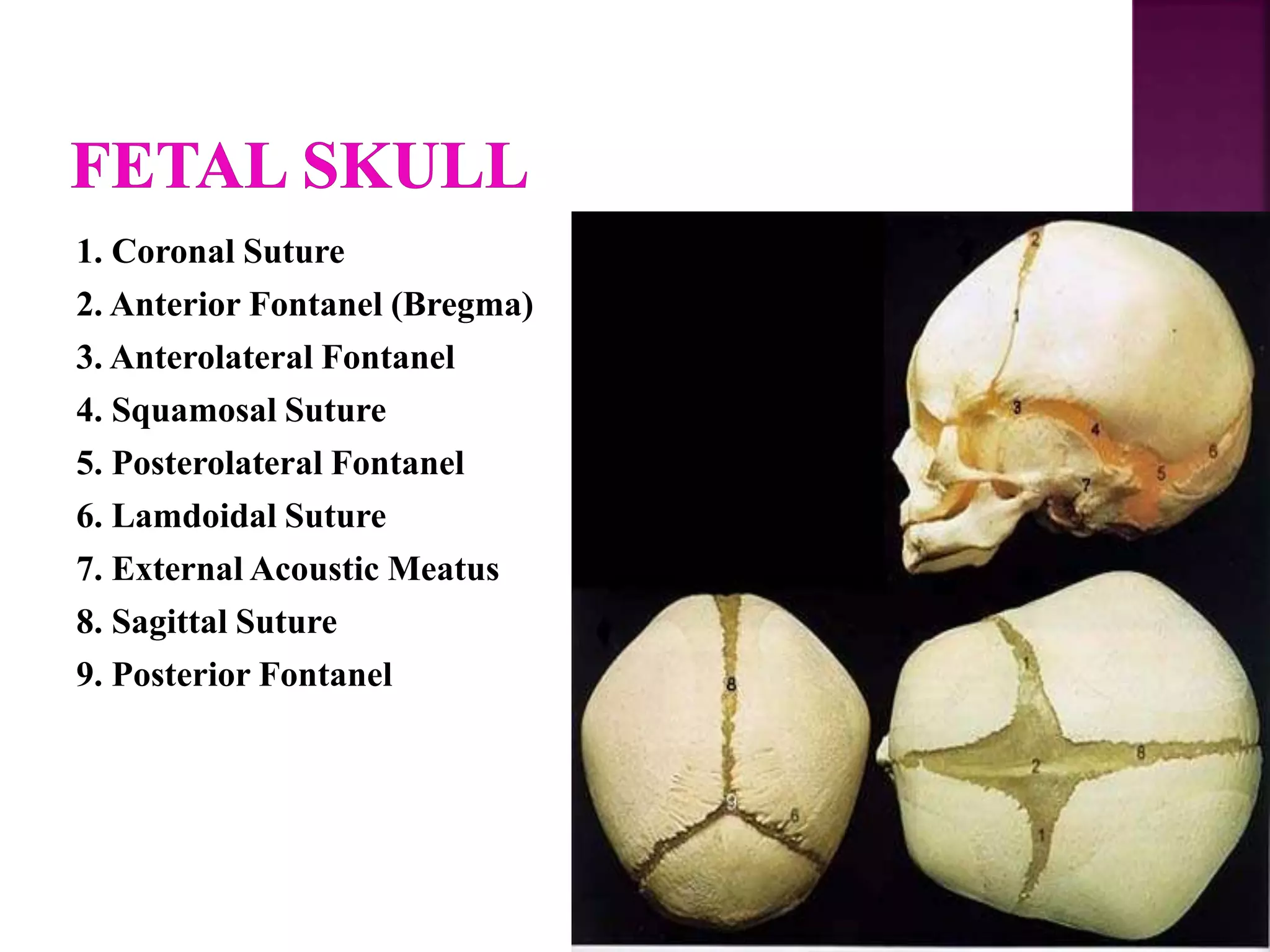
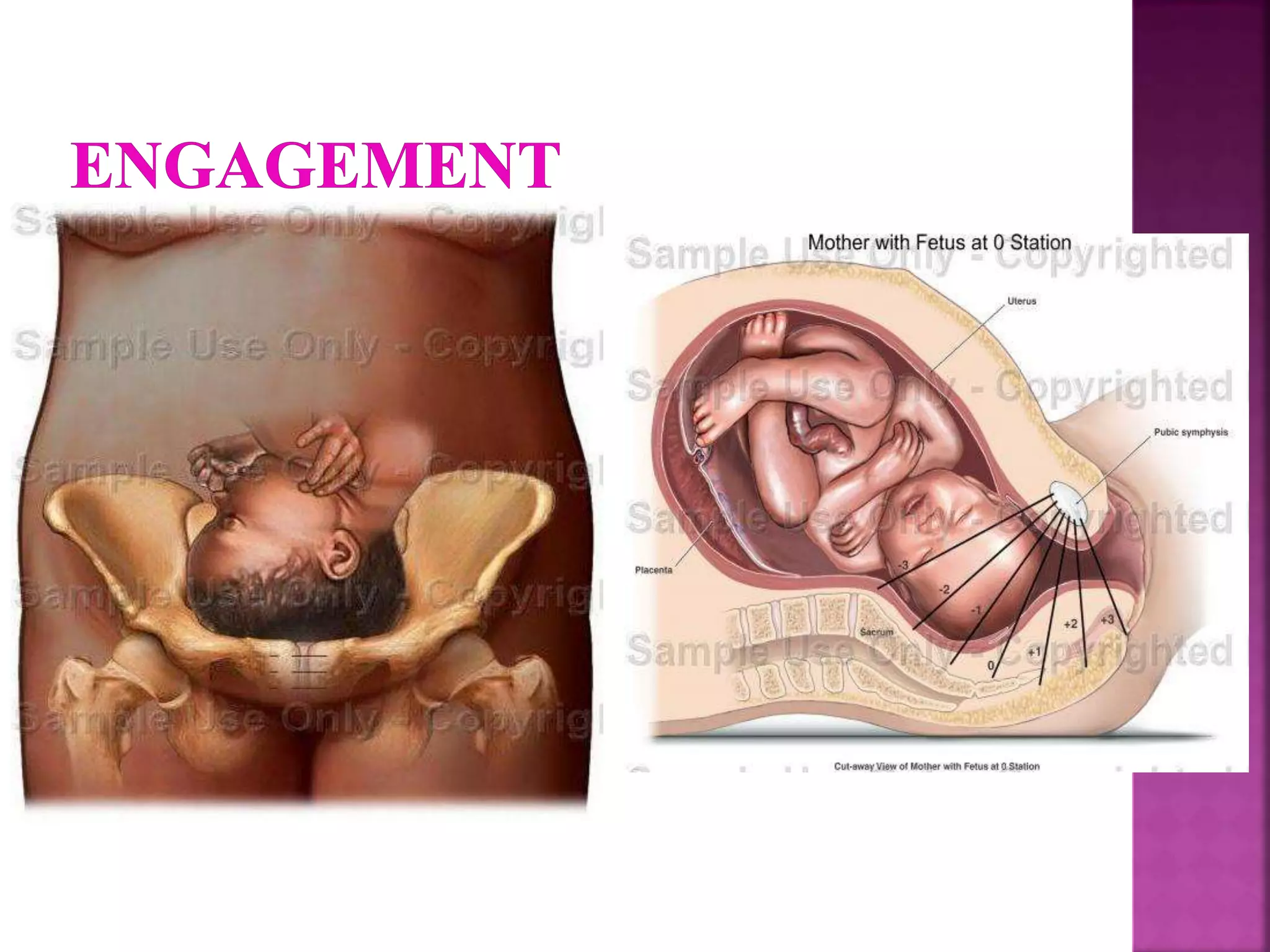



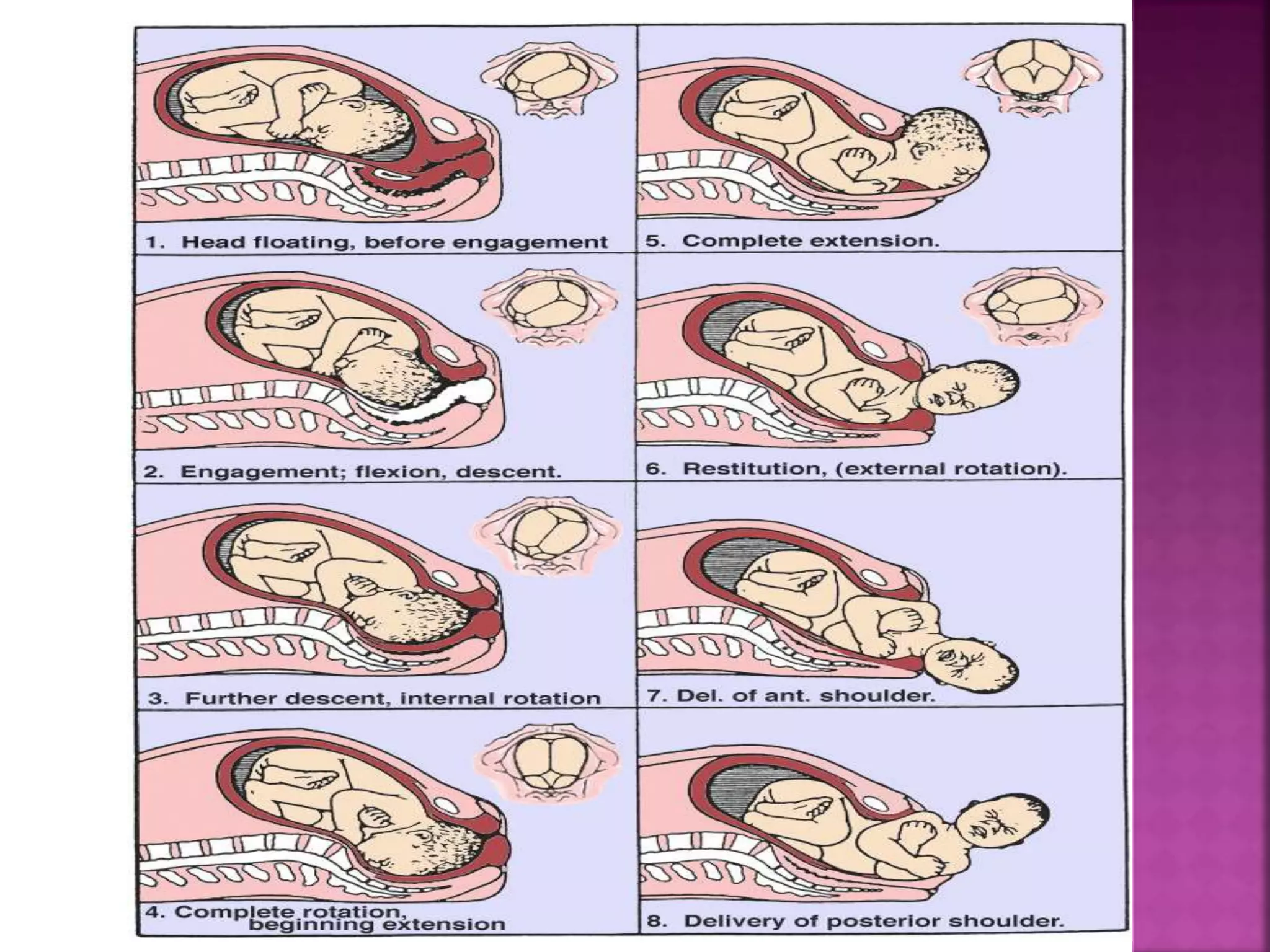

This document discusses the process of labor and delivery. It begins by defining labor as the series of contractions that expel the fetus, placenta, and membranes from the uterus through the vagina. It then discusses the three powers involved in delivery - the uterus, pelvic passages, and fetus. The document goes on to describe pelvic anatomy including types of pelvises and measurements. It concludes by outlining the normal mechanism of delivery, including engagement, descent, flexion, internal rotation, extension, restitution, external rotation, and shoulder and body delivery.























































































