• Contraceptive orfertility Regulating methods are preventive methods
to help women avoid unwanted pregnancies.
• They include all temporary and permanent measures to prevent
pregnancy.
• The presentapproach in family planning programmes is to
offer all methods from which an individual can choose
according to his needs and wishes and to promote family
planning as a way of life.
• Conventional contraceptives denote methods used that require
action at the time of coitus.
E.g. : Condoms , spermicides , etc .
5.
Spacing methods
Barriermethods
A) PHYSICAL METHODS
B) CHEMICAL METHODS
C) COMBINED METHODS
Intra-uterine devices
Hormonal methods
Post-conceptional methods
Miscellaneous
BARRIER METHODS
Occlusive methods:
Theaim of these methods is to prevent sperm from meeting
Ovum.
Eg: Male condom, female condom
Advantages :
Free from side effects associated with pills & IUD.
Protection from STD’s , pelvic inflammatory diseases & cancer
Cervix.
8.
Disadvantages
High degree ofmotivation
Less effective than pill or loop
They should be used consistently & carefully.
9.
INTRA UTERINE DEVICES
2types of IUDs
1. Nonmedicated 2. Medicated
1.Cu IUDs 2. Hormone Releasing
• Both types ( Medicated & Nonmedicated ) IUDs made up of
polyethylene or other polymers.
10.
• Non medicated/Inert/ First generation IUDs :
• Loops, spirals, coils, rings, bows etc.
12.
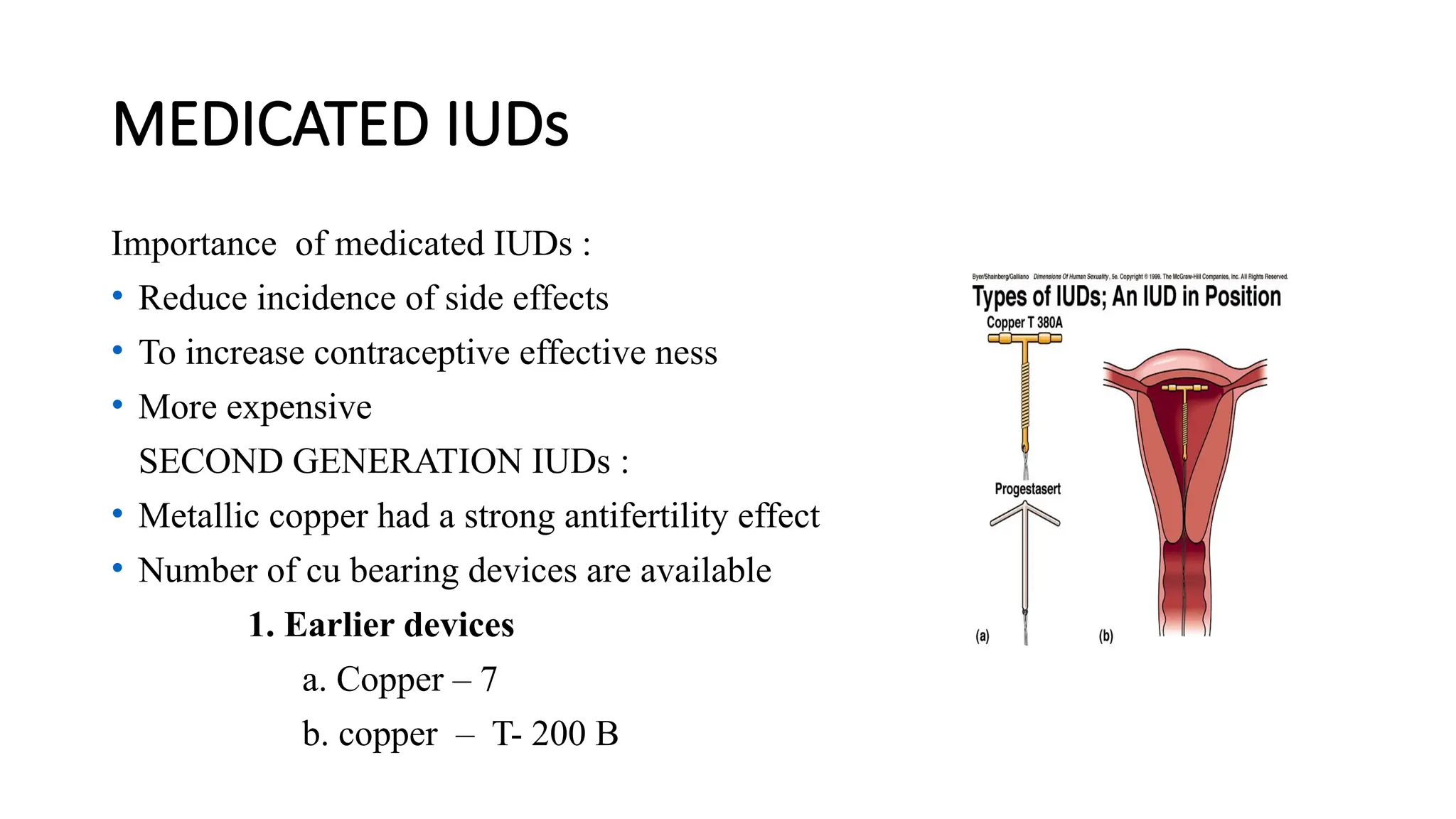
MEDICATED IUDs
Importance ofmedicated IUDs :
• Reduce incidence of side effects
• To increase contraceptive effective ness
• More expensive
SECOND GENERATION IUDs :
• Metallic copper had a strong antifertility effect
• Number of cu bearing devices are available
1. Earlier devices
a. Copper – 7
b. copper – T- 200 B
13.
2. Newer devices
a.variants of the T devices
i. T cu – 220C
ii. T cu – 380 A or Ag
b. Nova T
c. Multi load devices
i. ML – Cu -250
ii. ML – Cu- 375
Numbers represents the surface area of
the copper on the device (in. sq mm).
14.
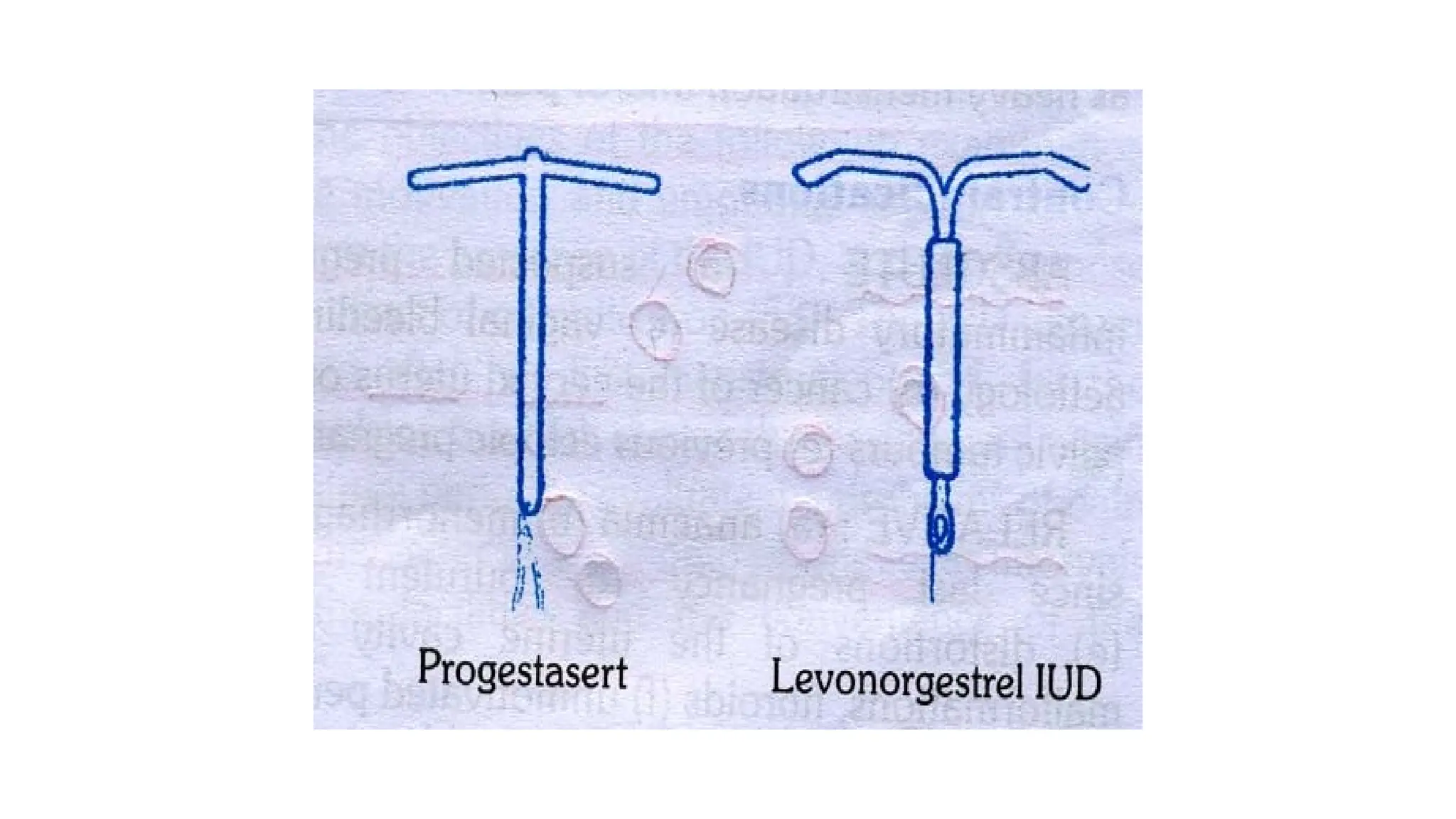
THIRD GENERATION IUD
•Most widely used hormonal devices are
1.Progestasert
• T shape device filled with 38 mg of progesterone
• It has direct effect on uterine lining, cervical mucus and sperms
• 2. Levonorgestrel (LNG – 20)
• T shaped device
• It has 1. low pregnancy rate
2. less number of ectopic pregnancies
3. Lower menstrual blood loss
4. Fewer days of bleeding
16.
MOA
• Foreign bodyreaction.
• Cellular and biochemical changes.
• Impair the viability of the gamete.
• Reduce the chances of fertilisation rather than implantation.
• Copper enhances the Cellular response in the endometrium.
• Affects the enzymes in the uterus.
• Alter biochemical composition ofcervical mucus.
• Hormonal devices increase viscosity of the cervical mucus.
17.
Advantages
• 1. Simplicity
•2. Insertion takes few minutes
• 3. Once inserted IUD stays in place as long as required
• 4. Reversible
• 5. In expensive
• 6. High continuation rates
• 7. Single act of motivation
• 8. Free of systemic side effects
18.
HORMONAL CONTRACEPTIVES
• Hormonalcontraceptives when properly used are the most effective
methods of contraception
• They provide the best means of ensuring spacing between one
childbirth and another
• GONADAL STEROIDES:
a. synthetic steroids: eg ethinyl oestradiol and mestranol.
b. synthetic progestogens: they are pregnanes , oestranes and
gonanes.
19.
CLASSIFICATION
a) ORAL PILLS
1.Combinedpills
2.Progestogen only pill
3.Post coital pill
4.Once a month pill
5.Male pill
b) DEPOT FORMULATIONS
1. Injectables
2. Subcutaneous implants
3. vaginal rings
20.
ORAL PILLS
1. Combinedpill:
It is one of the major spacing methods of contraception.It
contains 30-35 mcg of a synthetic oestrogen and 0.5 to 1
mcg of a progesterone.
The pill should be taken at a fixed time everyday.
21.
• The pillis given orally for 21 days starting on the 5th
day of menstrual
cycle followed by a break of 7 days during which menstruation occurs.
• This is called withdrawal bleeding.
• The department of family welfare , in the Ministry of Health and
Family Welfare Govt. of India has made available low dose of oral
pills – MALA-N and MALA-D.
22.
2. Progesterone onlypill
• It is called as minipill or micropill .it contains only progesterone which
is given in small doses through out the cycle.
• These pills have an increased pregnancy rate so not being used , but
can be used for women with cardiovascular problem and for those
with the risk factors for neoplasia.
23.
3. Post coitalcontraception:
It is used within 48 hrs of unprotected intercourse.
Two methods are available.
a) IUD: e.g. copper device
b) Hormonal: combine oc pill is used. It contains double dose of
the standard combined pill. 2 pills immediately followed by 2 pills
12 hours later.
For emergency contraception a women must take four instead of 2
in each dose.
24.
4. Once amonth long acting pill
• Quniestrol , a long acting estrogen is given in combination with a
short acting progesterone.
• Disadvantage: high pregnancy rate and irregular bleeding.
25.
5. Male pill:
Theapproach is
• a) preventing spermatogenesis.
b) interfering with sperm storage.
c) preventing sperm transport.
d) affecting the seminal fluid constitution.
• An ideal male contraceptive will decrease the sperm count while
leaving testosterone at normal values.
26.
Mode of actionof oral pill:
• Combined only pill prevents the release of ova from the ovary by
blocking the pituitary secretion of gonadotropin.
• Progesterone only pills render the cervical mucus thick and
scanty and inhibit the sperm penetration.
27.
Effectiveness :
• Iftaken according to the prescribed regimen oral contraceptives of
the combined type are 100% effective.
• It is also influenced by drugs – rifampicin, phenobarbital, ampicillin.
28.
BENEFICIAL EFFECTS
Contraceptive benefits-prevention of unwanted pregnancy (failure rate-
0.1per 100 women year).
Non contraceptive benefits-
a. relief of:
menorrhagia (50% ),
dysmenorrhoea (40% ),
premenstrual tension syndrome,
mittleschmerz syndrome.
b. improvement of:
iron def. anemia,hirsutism,
acne, endometriosis, autoimmune disorders of
thyroid, rheumatoid arthritis.
29.
c. Marked reductionin: pelvic inflammatory disease, benign breast
cancer, ectopic pregnancy, fibroid uterus, functional ovarian cysts,
carcinoma of ovary (40%) carcinoma of endometrium (50% )
protection against osteoporosis.
30.
b) DEPOT FORMULATIONS
•Injectable contraceptives, sub dermal implants and vaginal
rings come in this category.
1. Injectable contraceptives:
There are two types:
PROGESTAGEN ONLY INJECTABLES:
• (a) DMPA: Depot medroxy - progesterone acetate.
• Dose is i.m injection of 150mg every 3months.
31.
• It issafe effective and an acceptable contraceptive.
• Acceptable in the postpartum period as a means of spacing.
• Side effects: weight increase, irregular menstrual bleeding.
32.
(b) NET-EN
• Norethisteroneenantate is given as i.m injection dose of
200mg. every 60 days.
• Contraceptive action is by inhibiting ovulation and
progesterogenic effects on cervical mucus.
ADMINISTRATION:
• Both DMPA ,NET-EN should be given during first five days of
menstrual period.
33.
B. COMBINED INJECTABLE:
• They contain a progestogen and an oestrogen.
• Given at monthly intervals.
• Act by suppressing ovulation ,cervical mucus is affected
mainly by progestogen and inhibits sperm penetration.
• CONTRAINDICATIONS: confirmed or suspected pregnancy;
past or present evidence of thromboembolic disorders;
cerebrovascular or coronary artery disease; focal migraine;
malignancy of breast and diabetes with vascular
complications.
34.
2. SUBDERMAL IMPLANTS:
•Norplant : it consists of 6 silastic capsules containing 35mg of
levonorgesterel.
• The capsules are implanted beneath the skin of forearm or
upper arm.
• Effective contraception is provided for 5 years.
35.
3. VAGINAL RINGS
Vaginalrings containing levonorgesterel are highly effective.
• The hormone is slowly absorbed through the vaginal mucosa
, bypassing the digestive tract and liver and allowing a
potentially lower dose.
• The ring is worn in the vagina for 3 weeks and removed for
the 4th
week.