This document discusses breech presentation, including its definition, types, diagnosis, and management. Some key points:
- Breech presentation is when the buttocks or lower limbs present first. It occurs in 3.5% of term deliveries and up to 25% of preterm deliveries.
- Types include complete breech, frank breech, and footling breech. Diagnosis is made through inspection, palpation, auscultation, and ultrasound.
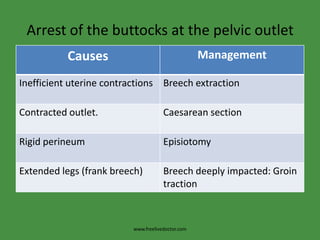
- Management options are external cephalic version, vaginal delivery for some cases, or caesarean section which is recommended for complicated breeches or large babies. Vaginal delivery carries risks of complications for













































![Breech presentation [autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/breechpresentationautosaved-211128120250-thumbnail.jpg?width=640&height=640&fit=bounds)