Downloaded 3,328 times











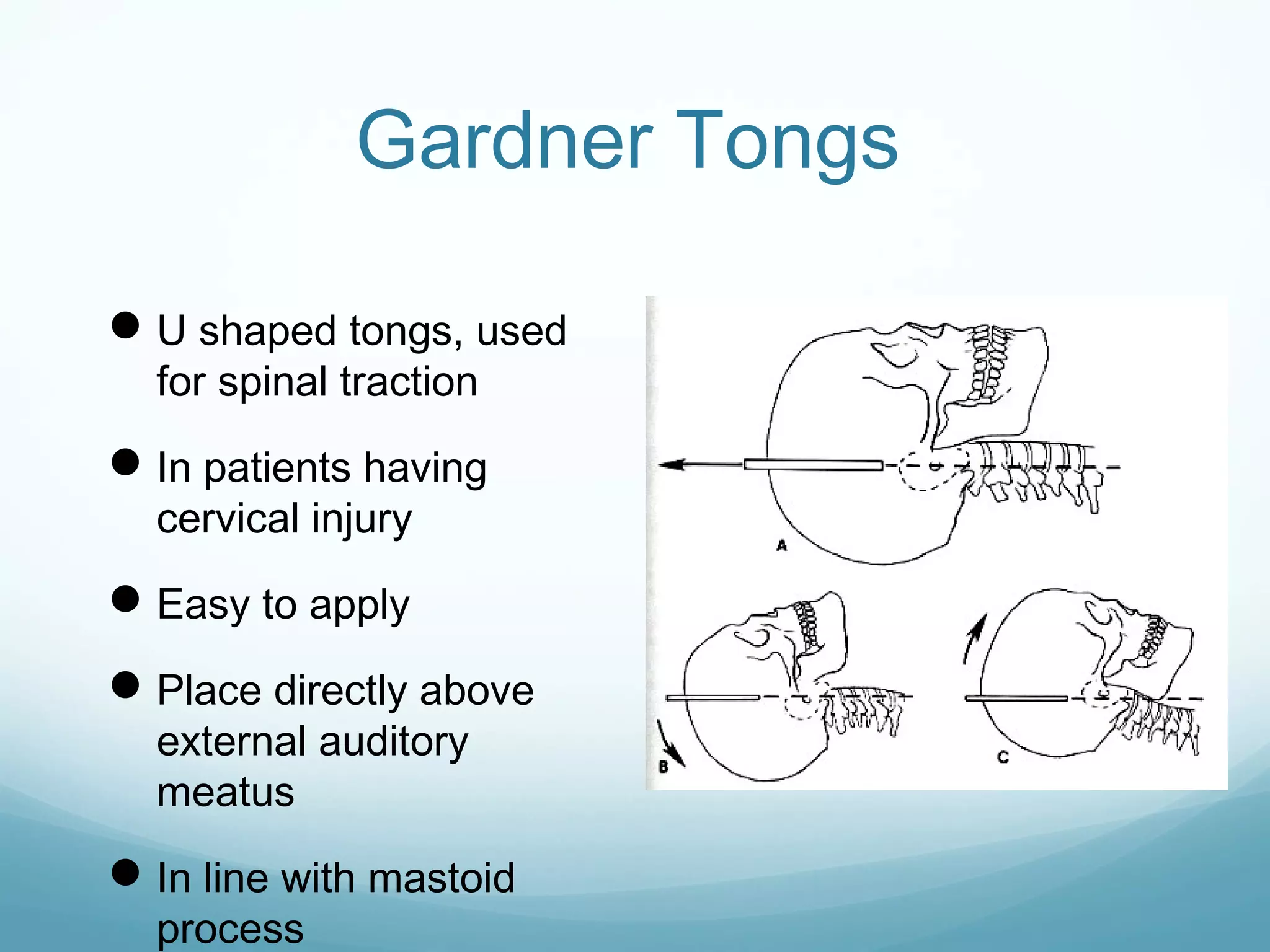
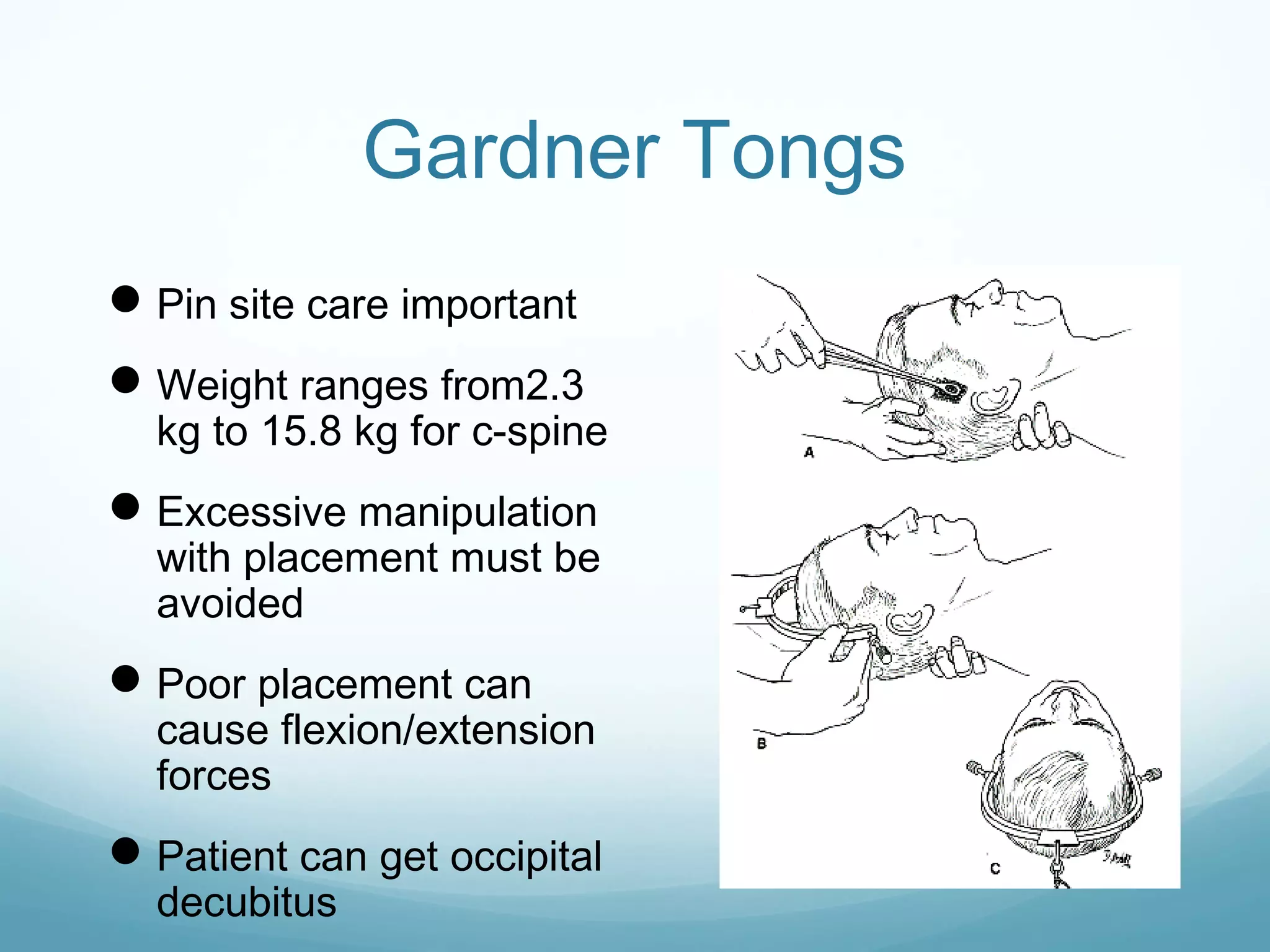










This document provides an overview of traction in orthopedics. It discusses the history and types of traction, including skin traction and skeletal traction. Various traction methods are described for different body parts, including Buck's traction for the femur, olecranon traction for the humerus, and Gardner tongs for spinal traction. Both advantages and disadvantages of traction are reviewed. Key aspects like pin placement, weight limits, and complications are covered.











































































