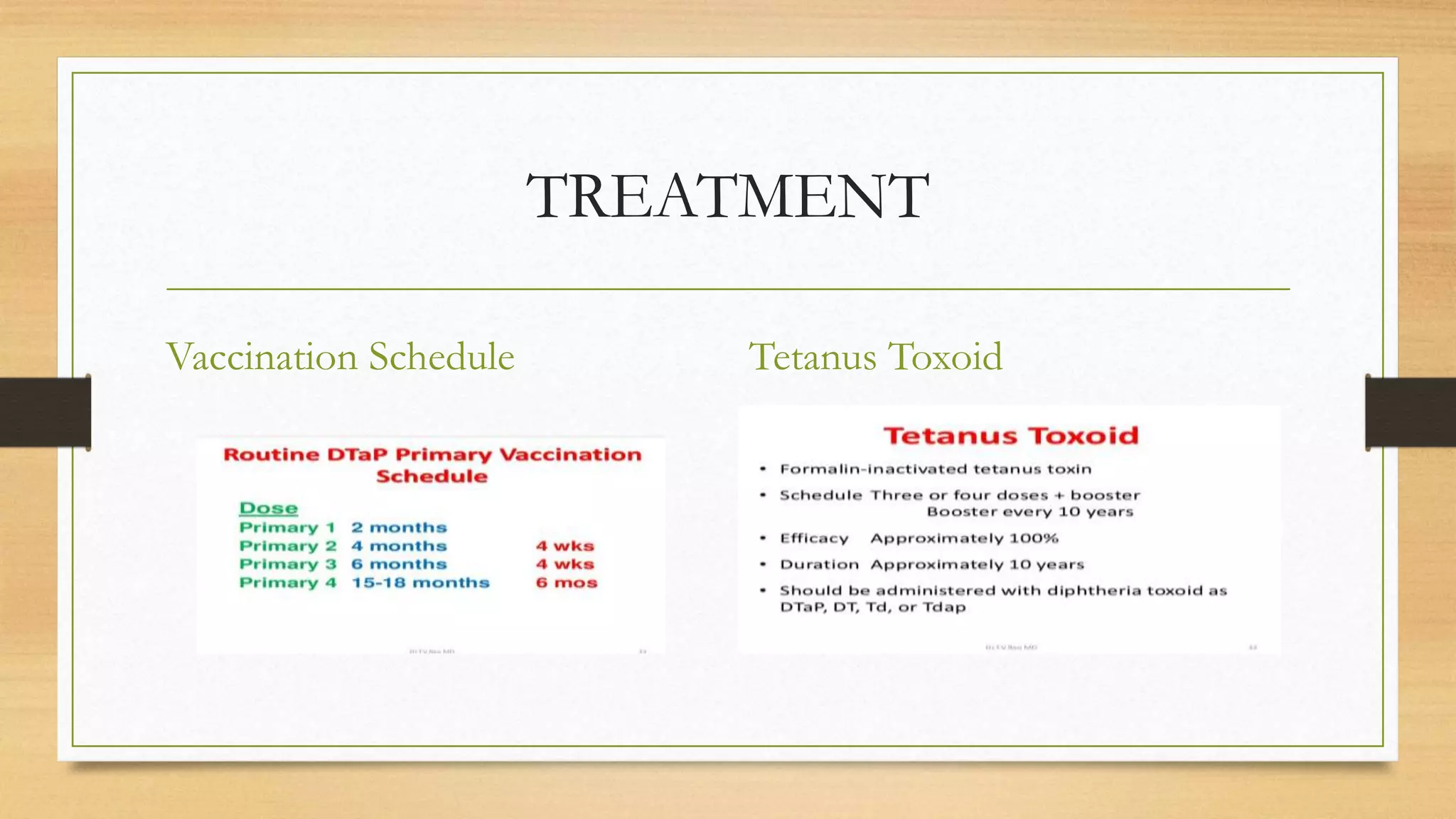
Tetanus is a neurological disease caused by the bacterium Clostridium tetani, characterized by painful muscle contractions and spasms, especially in the jaw and neck. It is preventable through vaccination, yet still poses significant health risks globally due to its wide presence in soil and in unvaccinated individuals. Effective management includes immunization, wound care, and antibiotics, although tetanus remains a serious condition with high morbidity and mortality rates.