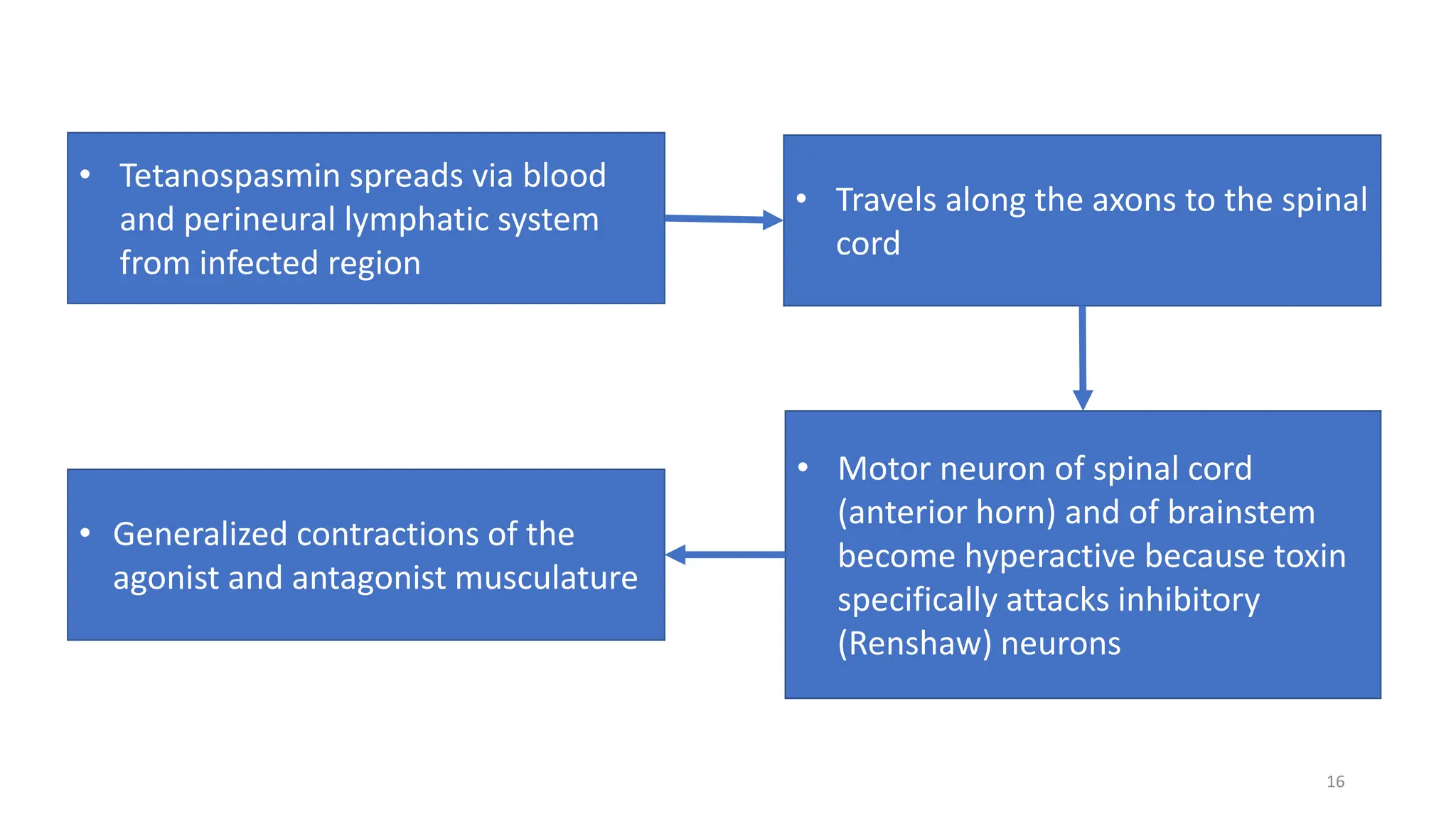
The document provides a comprehensive overview of tetanus, including its causative agent, epidemiology, clinical features, types, diagnosis, treatment, and prevention strategies. Tetanus is primarily caused by Clostridium tetani and is preventable through vaccination, with significant efforts made in Nepal leading to the elimination of neonatal tetanus since 2005. The document emphasizes the importance of addressing host factors, transmission routes, and effective management protocols to enhance patient care.