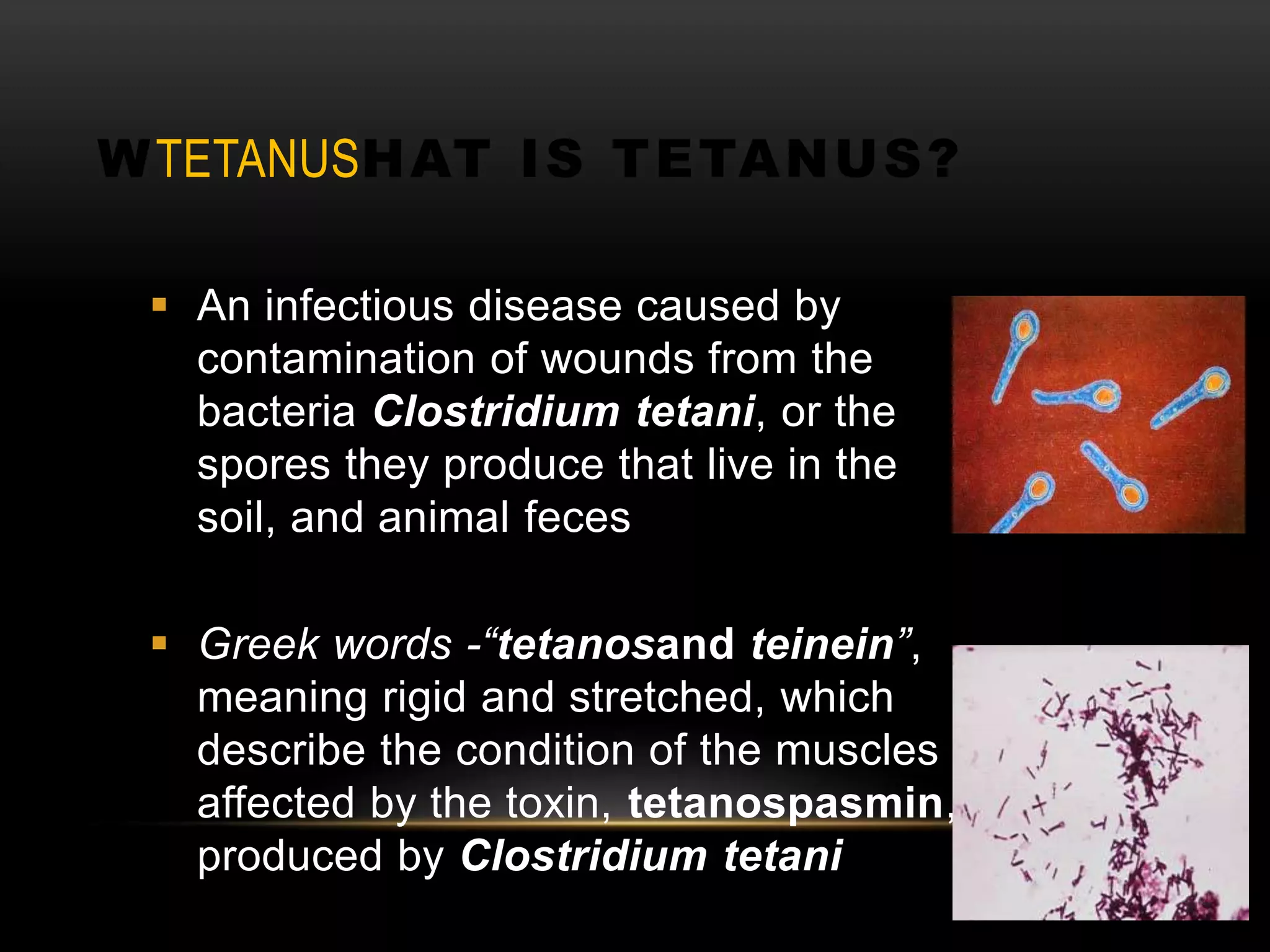
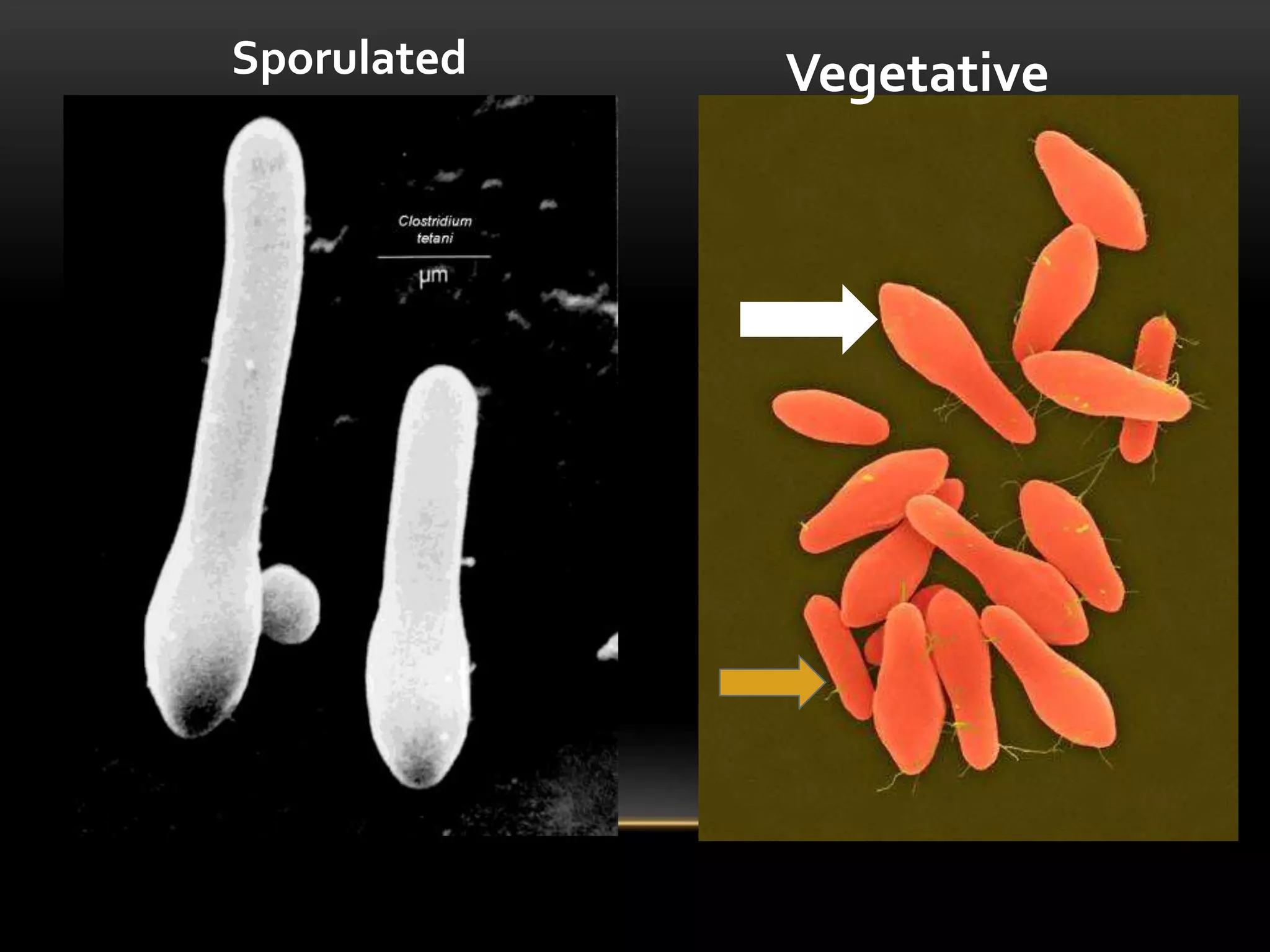
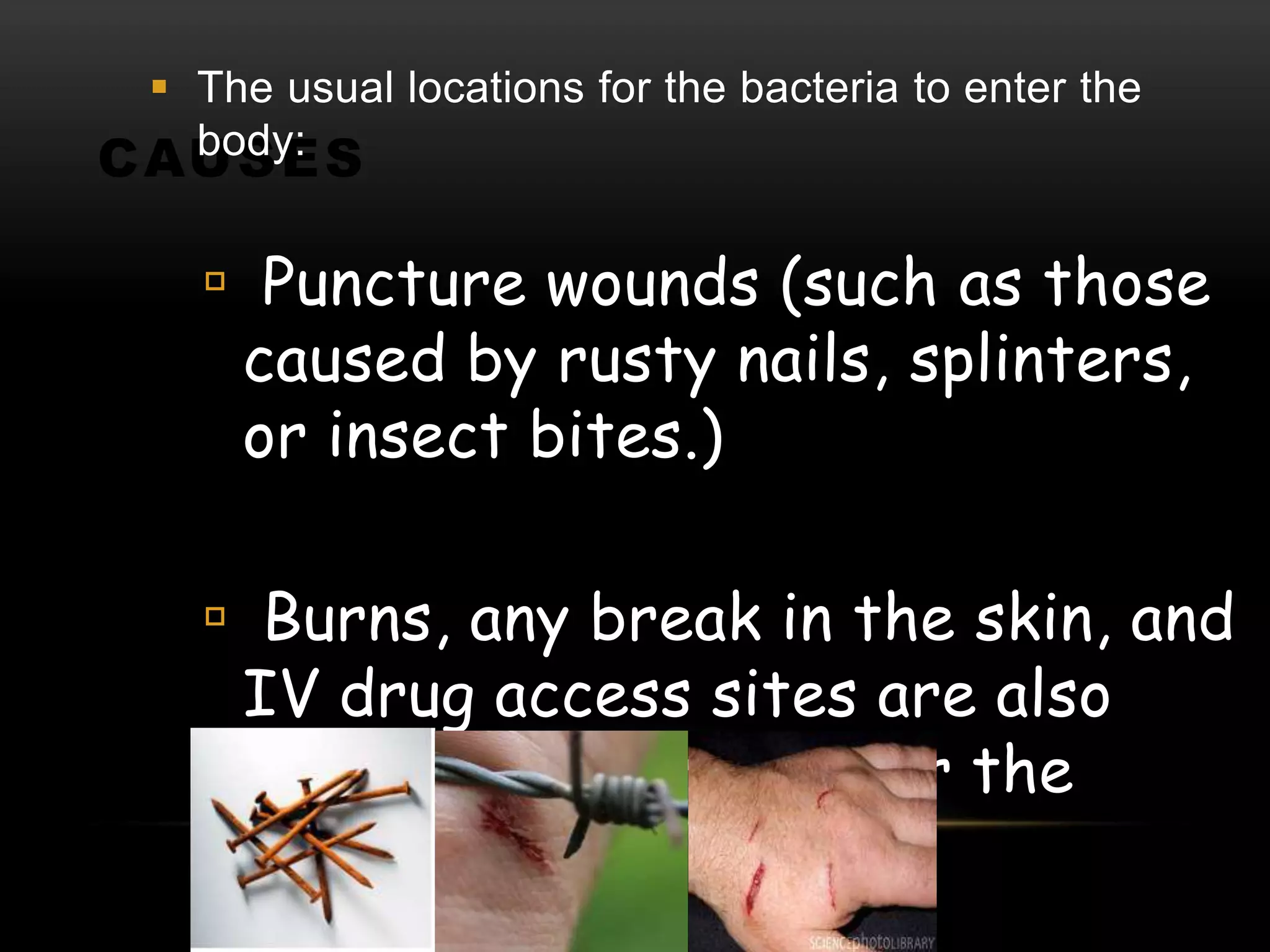
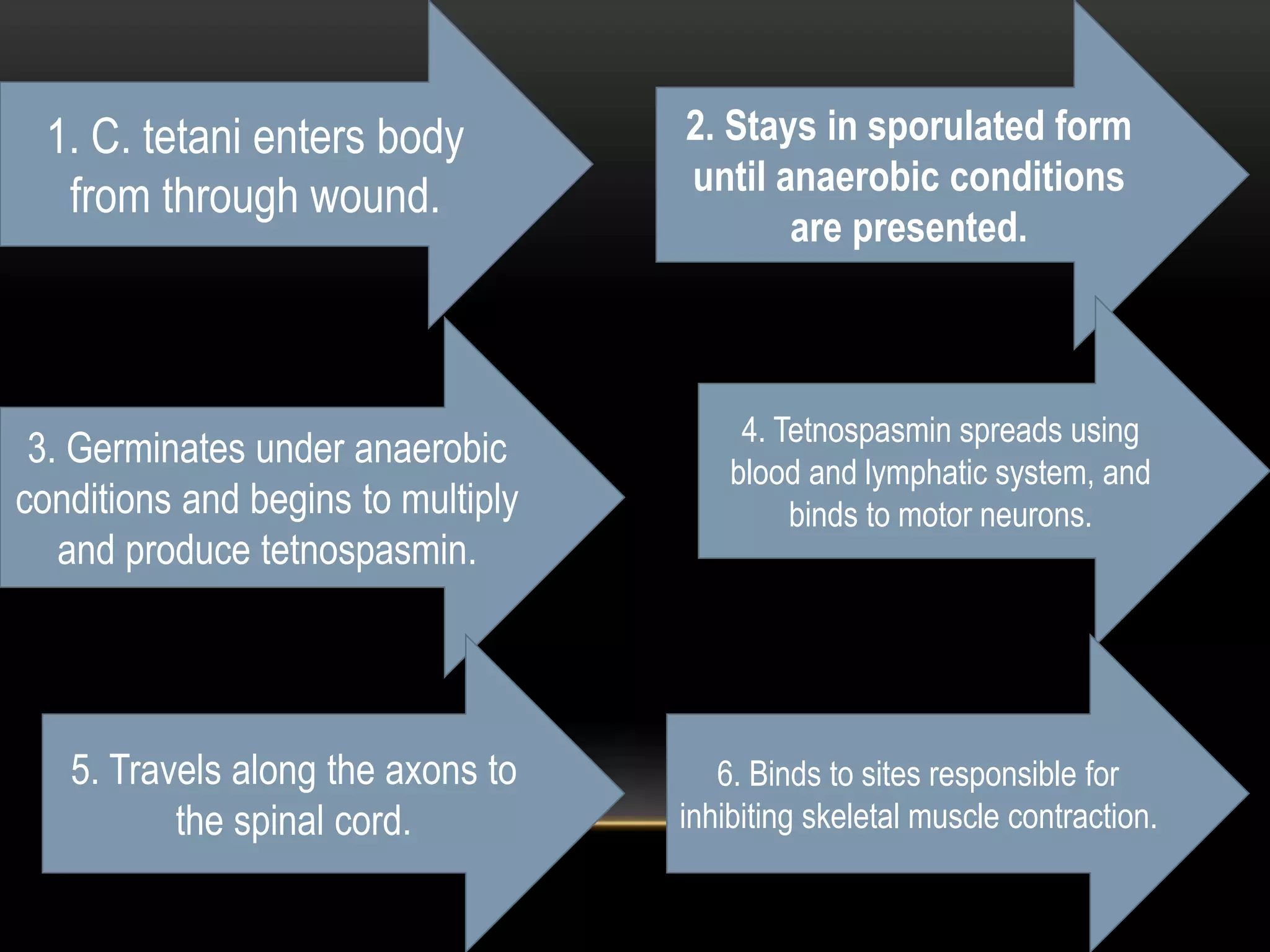
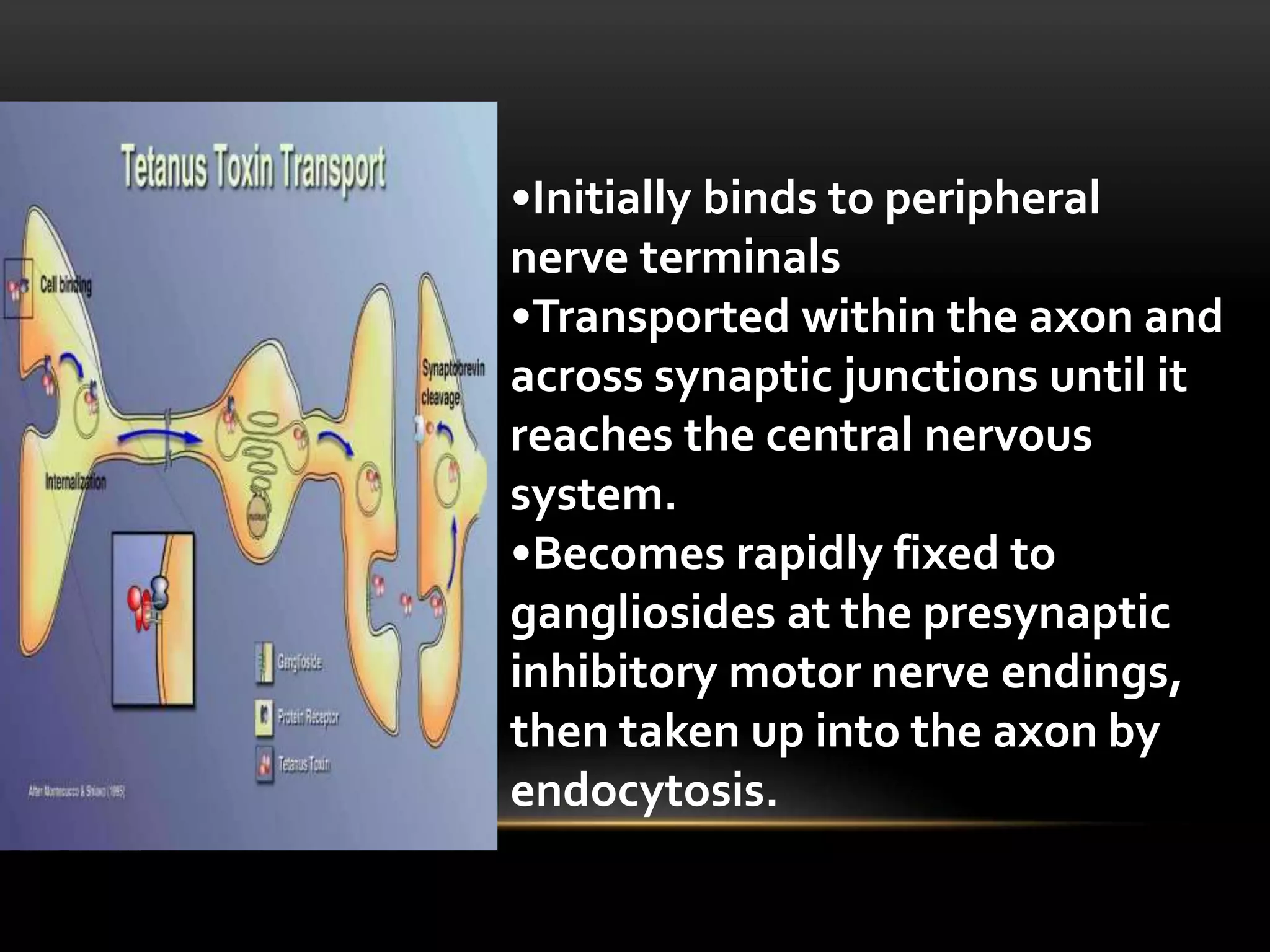
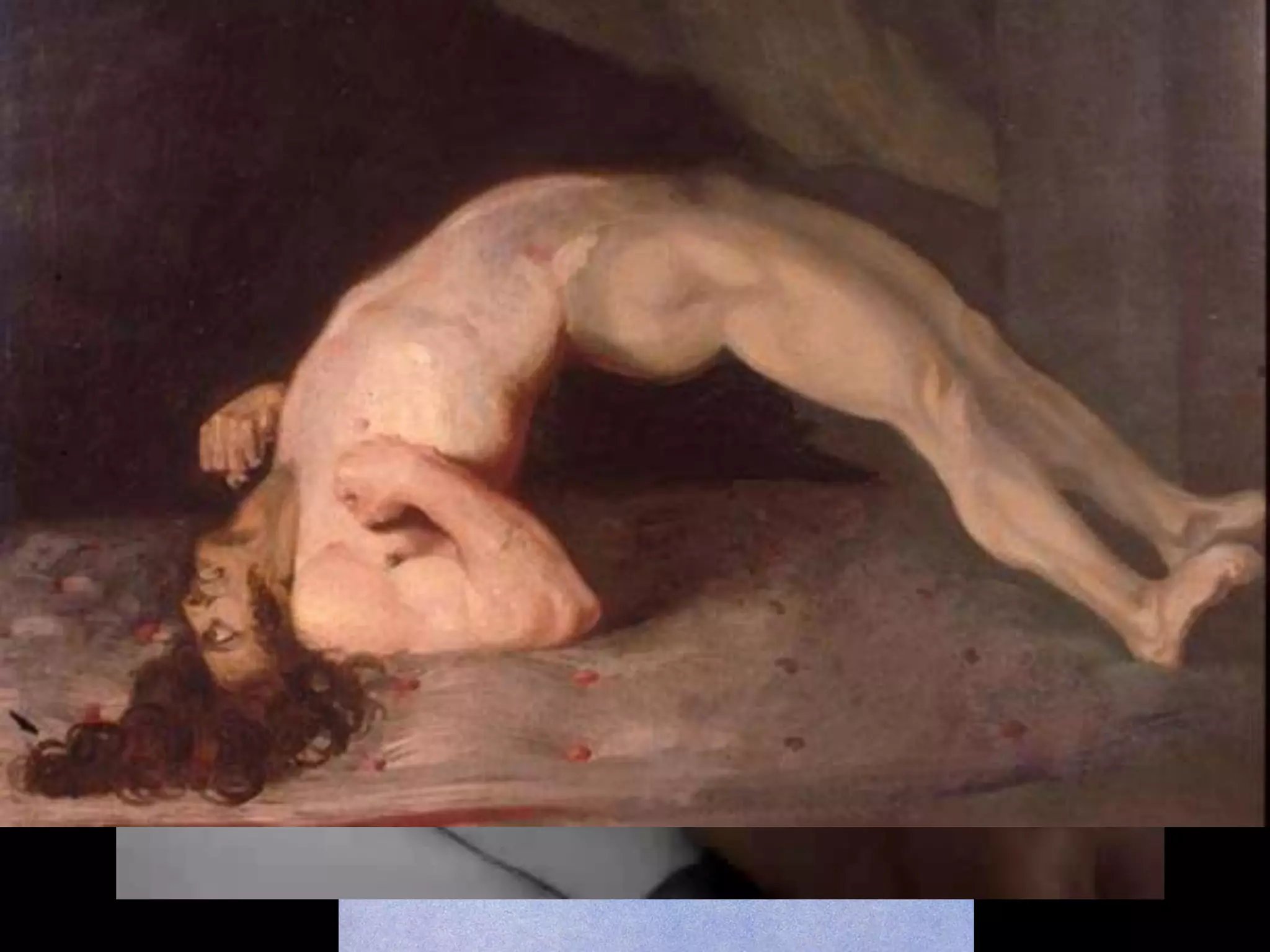
Tetanus is caused by the bacteria Clostridium tetani entering the body through wounds and producing a toxin that causes painful muscle spasms. It is found worldwide in soil and animal waste. The spores can live for years in the body until an injury provides an anaerobic environment for the bacteria to grow. The toxin travels up motor neurons to the spinal cord where it blocks inhibitory neurotransmitters, causing sustained muscle contractions. Symptoms include lockjaw, arching of the back, and risus sardonicus. Treatment involves wound cleaning, antibiotics, antitoxin antibodies, and supportive care. Tetanus is preventable through active immunization with the tetanus toxoid vaccine as part of