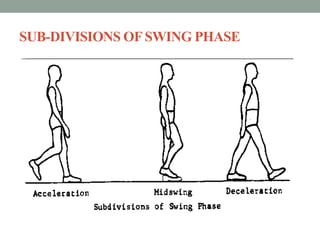
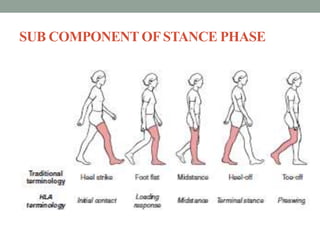
This document provides an overview of gait disorders, including normal gait cycle components and subdivisions, physiological and anatomical aspects of gait, common causes and types of abnormal gait, clinical symptoms and examination of gait. Key points covered include definitions of stance and swing phases, centers of pressure and gravity, neurological structures involved in locomotion, epidemiology of gait disorders in older adults, gait abnormalities due to weakness, spasticity, sensory deficits and imbalance. Classification of gait patterns such as myopathic, neurogenic, sensory ataxia, vestibular imbalance and spastic hemiparetic gaits are described.








































































![DUAL AND TRIPLE ANTITHROMBOTIC THERAPY FOR SECONDARY STROKE [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/dualandtripleantithrombotictherapyforsecondarystrokeautosaved-230904113552-c3502b37-thumbnail.jpg?width=640&height=640&fit=bounds)

































