Download to read offline
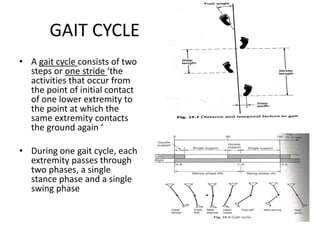
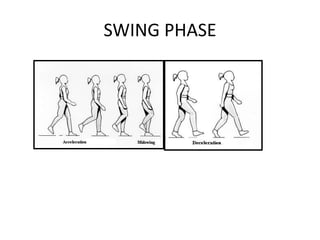
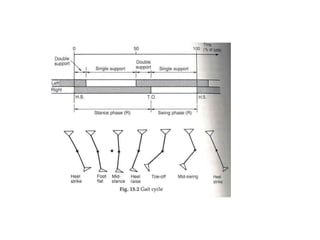
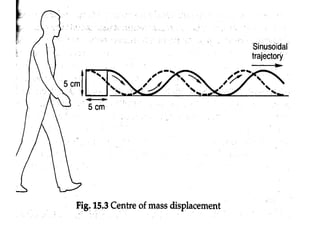
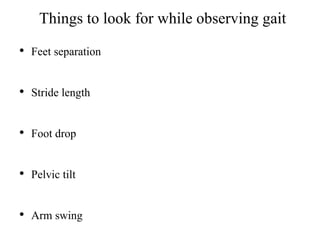

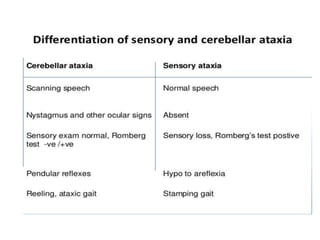
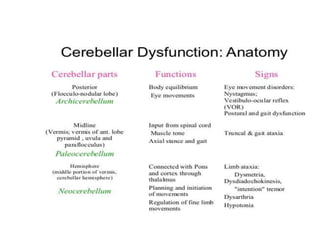
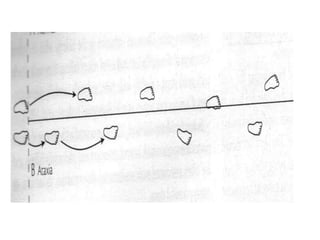
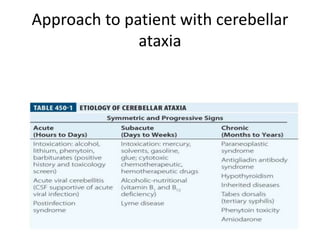
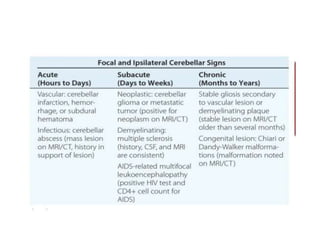
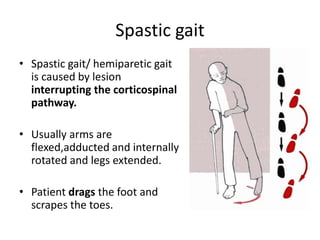
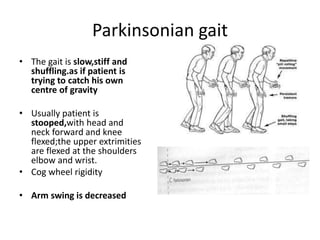
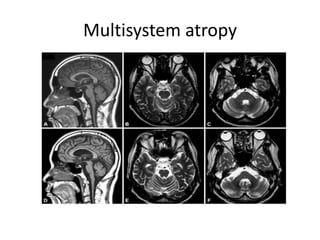


This document discusses gait disorders and their causes. It defines normal gait and describes the gait cycle. It then discusses various types of abnormal gaits such as sensory ataxia caused by disturbances in sensory input, cerebellar ataxia presenting with wide-based staggering gait, and spastic gait caused by lesions interrupting the corticospinal pathway. It also covers parkinsonian gait, multisystem atrophy presenting with features of both parkinsonism and cerebellar ataxia, and spinocerebellar ataxia which is an inherited condition. Various causes of acquired and inherited ataxias are described.




















































![ivct and ivrt IN CARDIAC CYCLE [Autosaved] .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/ivctandivrtautosaved-copy-250829033609-78e4fe1b-thumbnail.jpg?width=640&height=640&fit=bounds)


































