





![Mechanism of injury :
Direct traumatic impact or fall on the shoulder 87% .
Direct impact to clavicle 07% .
Fall on outstretched hand 06% .
From fall on the side .
Vigorous muscle contraction , seizures [rare] .
Pathological fracture [rare] .](https://image.slidesharecdn.com/claviclefracture-150405113828-conversion-gate01/75/Clavicle-fracture-8-2048.jpg)

![Most common causes are :
Road traffic accident [RTA]
Sporting injuries](https://image.slidesharecdn.com/claviclefracture-150405113828-conversion-gate01/75/Clavicle-fracture-10-2048.jpg)
![Allman classification : according to site of
fracture :
group 1: Fracture mostly occur in the
middle one third of clavicle 80% .
group 2: The fractures of outer third is 15% .
Fractures involving the acromioclavicular joint 28% .
group 3: fracture of inner [medial] third 5% .](https://image.slidesharecdn.com/claviclefracture-150405113828-conversion-gate01/75/Clavicle-fracture-11-2048.jpg)








![Diagnosis :
- Clinical picture examination .
investigation :
x-ray [AP view ] :
# is usually in middle third, outer fragment below
the inner .
#of outer third may be missed .
CT scan : useful for non union assessment .
arteriography : if vascular injury suspected .](https://image.slidesharecdn.com/claviclefracture-150405113828-conversion-gate01/75/Clavicle-fracture-20-2048.jpg)








![Complication:
late :
Malunion .
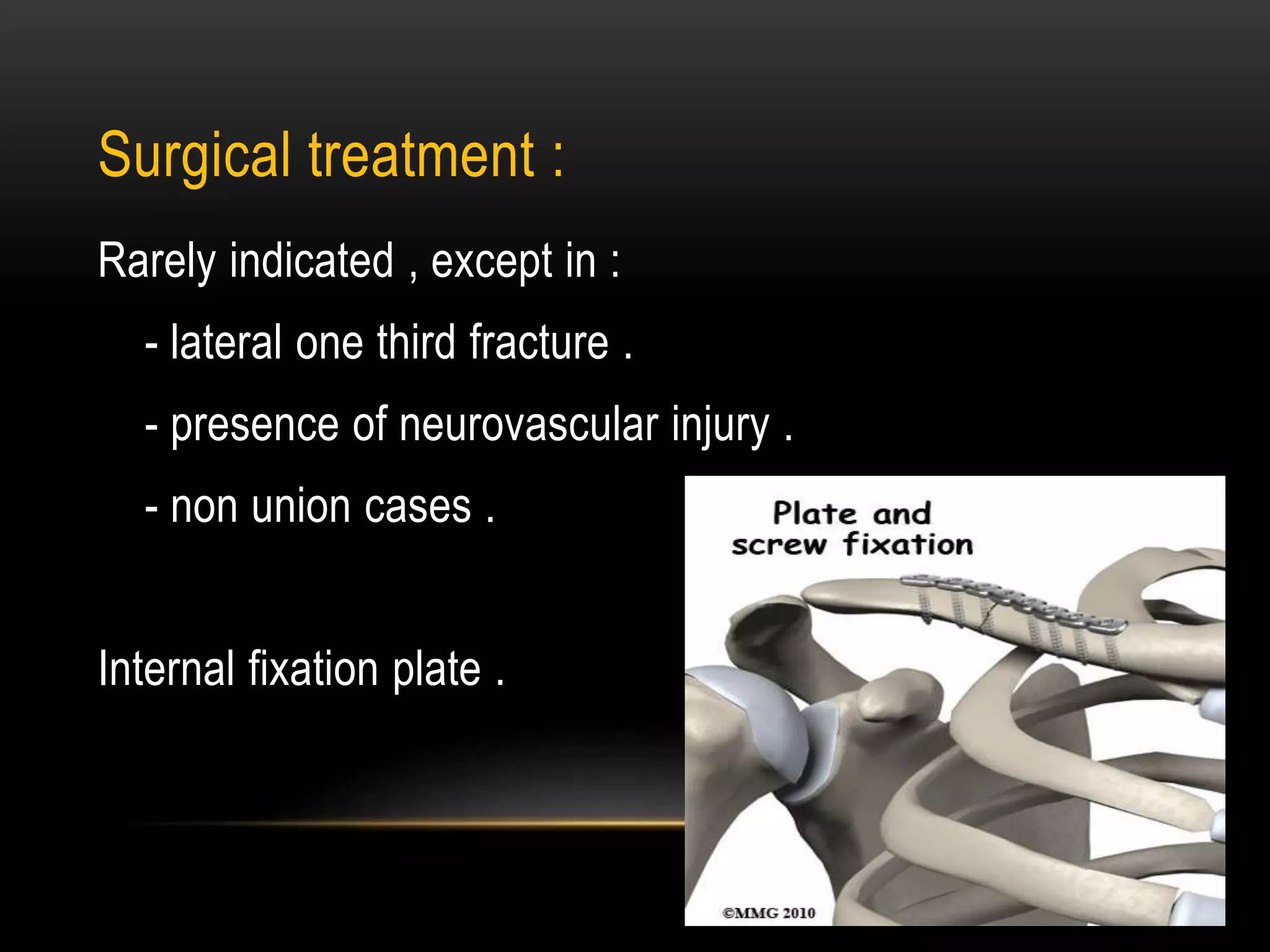
Ununion : treated by internal fixation and bone grafting .
Neurovascular injury [rare] . .
Stiffness of shoulder in elderly .
Ulnar neuropathy .
Refracture .
Early : [subclavian or carotid artery injury
,pneumothorax and hemothorax ,brachial injury ]](https://image.slidesharecdn.com/claviclefracture-150405113828-conversion-gate01/75/Clavicle-fracture-31-2048.jpg)












![Diagnosis :
After initial assessment , according to advanced trauma
life support [ATLS] principles , radiograghic evaluation is
indicated as soon as possible as patient stable .
X – ray :
Anteroposterior view lateral axillary view .
C T scan :is useful in glenoid or body # . .](https://image.slidesharecdn.com/claviclefracture-150405113828-conversion-gate01/75/Clavicle-fracture-46-2048.jpg)














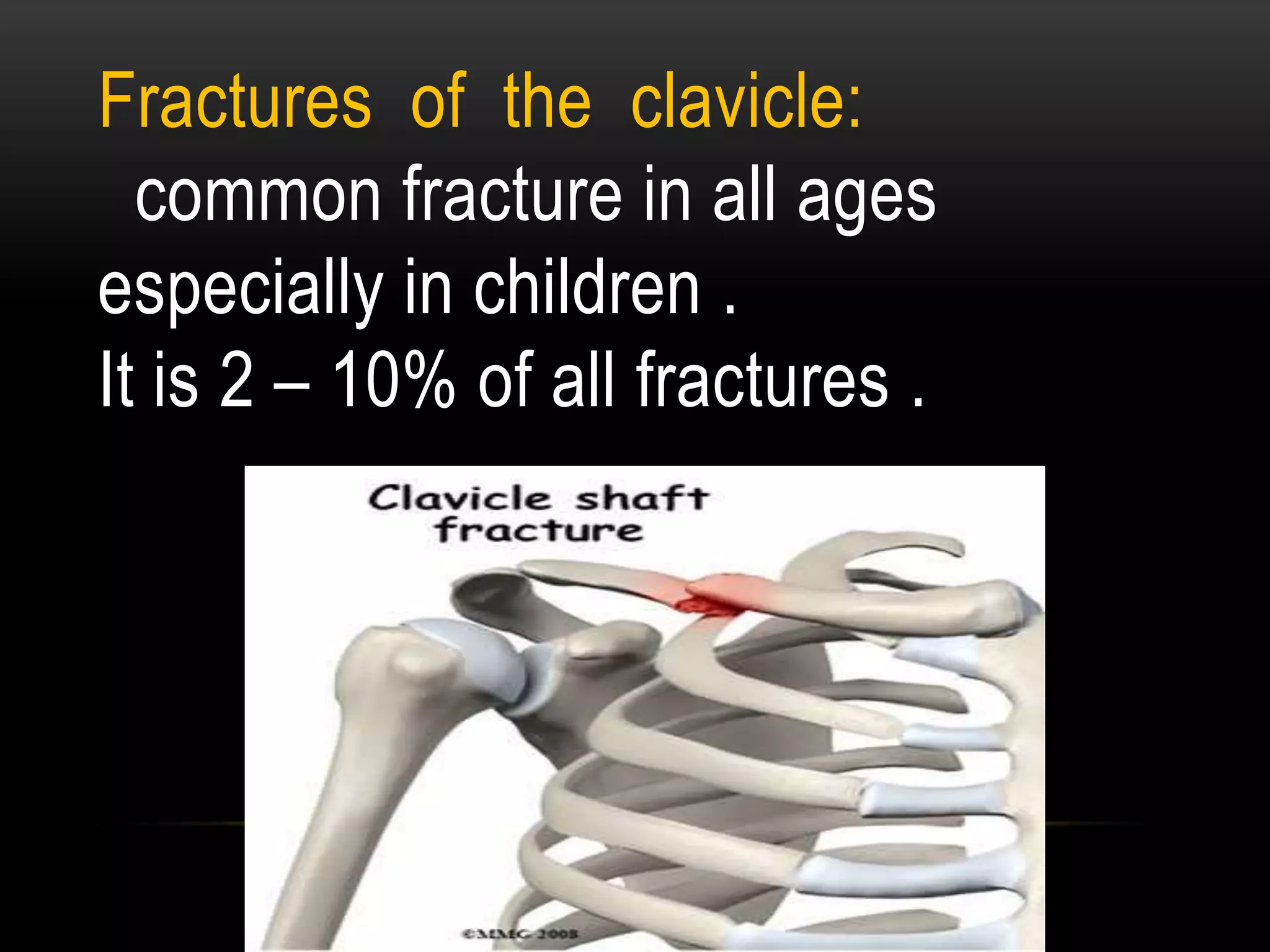
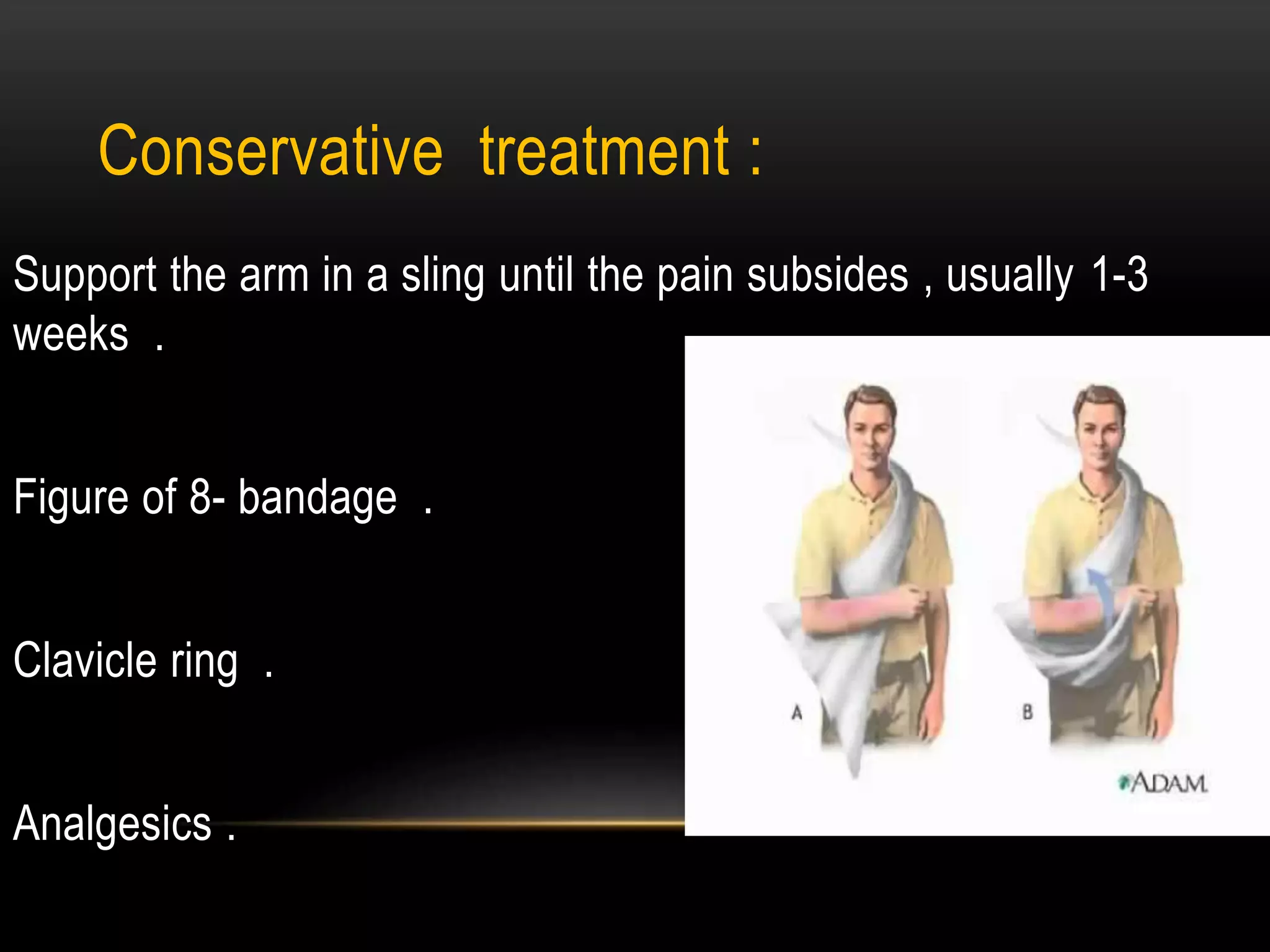
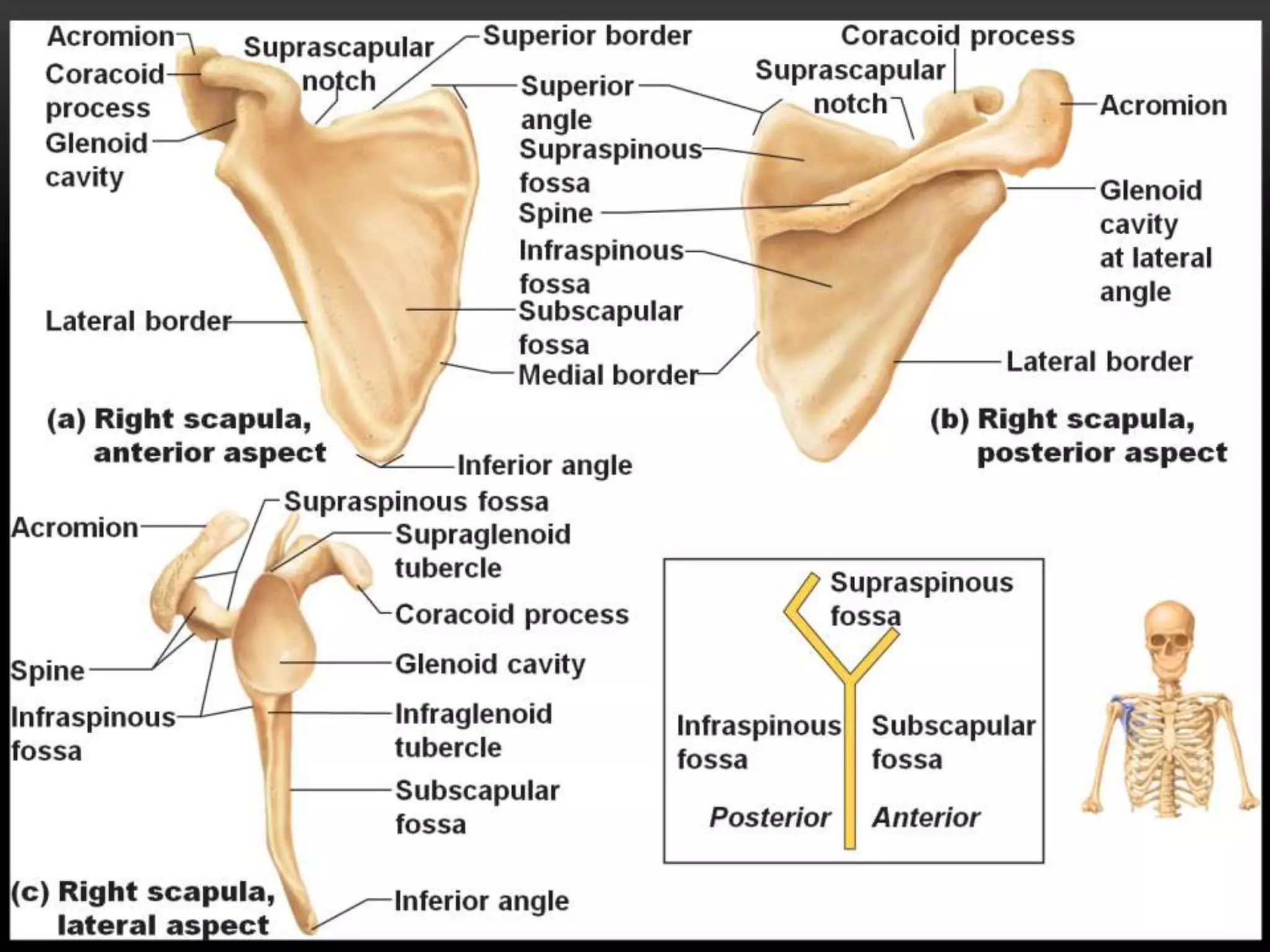
1. Fractures of the clavicle and scapula are uncommon but can result from high-energy trauma. 2. Clavicle fractures most commonly occur in the middle third and are usually treated conservatively with sling immobilization. 3. Scapula fractures involve the body, neck, glenoid, coracoid, or acromion and are often associated with life-threatening injuries requiring assessment by ATLS protocols. Most are also treated initially with sling immobilization.























































































