This document summarizes the diagnosis and management of scapula fractures. It discusses the anatomy, mechanisms of injury, classification systems, treatment indications, surgical approaches, complications, and recent literature. The key points are that scapula fractures often have associated injuries requiring evaluation, displacement or angulation greater than certain thresholds are indications for surgery, and internal fixation through a posterior approach typically yields good functional outcomes with low complication rates.
Introduction to scapula fractures, basic anatomy, importance, and an outline of key topics such as injury mechanisms, diagnosis, and treatment.
Common mechanisms of scapula fractures including direct trauma and high-energy injuries, with associated injuries occurring in 61%-98% of cases.
Clinical signs of scapula fractures and radiological evaluation methods, including various imaging views and the necessity of a CT scan.
Detailed anatomical classifications including OTA/AO and Ideberg classification, along with specific fracture types like glenoid and coracoid.Indications for surgery based on fracture types, displacements greater than 1 cm, and associated injuries requiring operative intervention.
Overview of complications linked to scapula fractures, including nerve injuries, malunions, and issues post-operative treatment.
Various surgical techniques and approaches including anterior, superior, and posterior methods for optimal exposure and fixation.
Information on post-operative treatment outcomes, complications, and effective management strategies based on recent literature.Take-home messages addressing associated injuries, radiological evaluations, surgical guidelines, and minimizing complications to improve patient outcomes.
Scapula fracture diagnosisand
management.
SEMINAR.
By: Dr Hemant Bansal
MS ,DNB Orthopedics.
AIIMS NEW DELHI,INDIA
2.
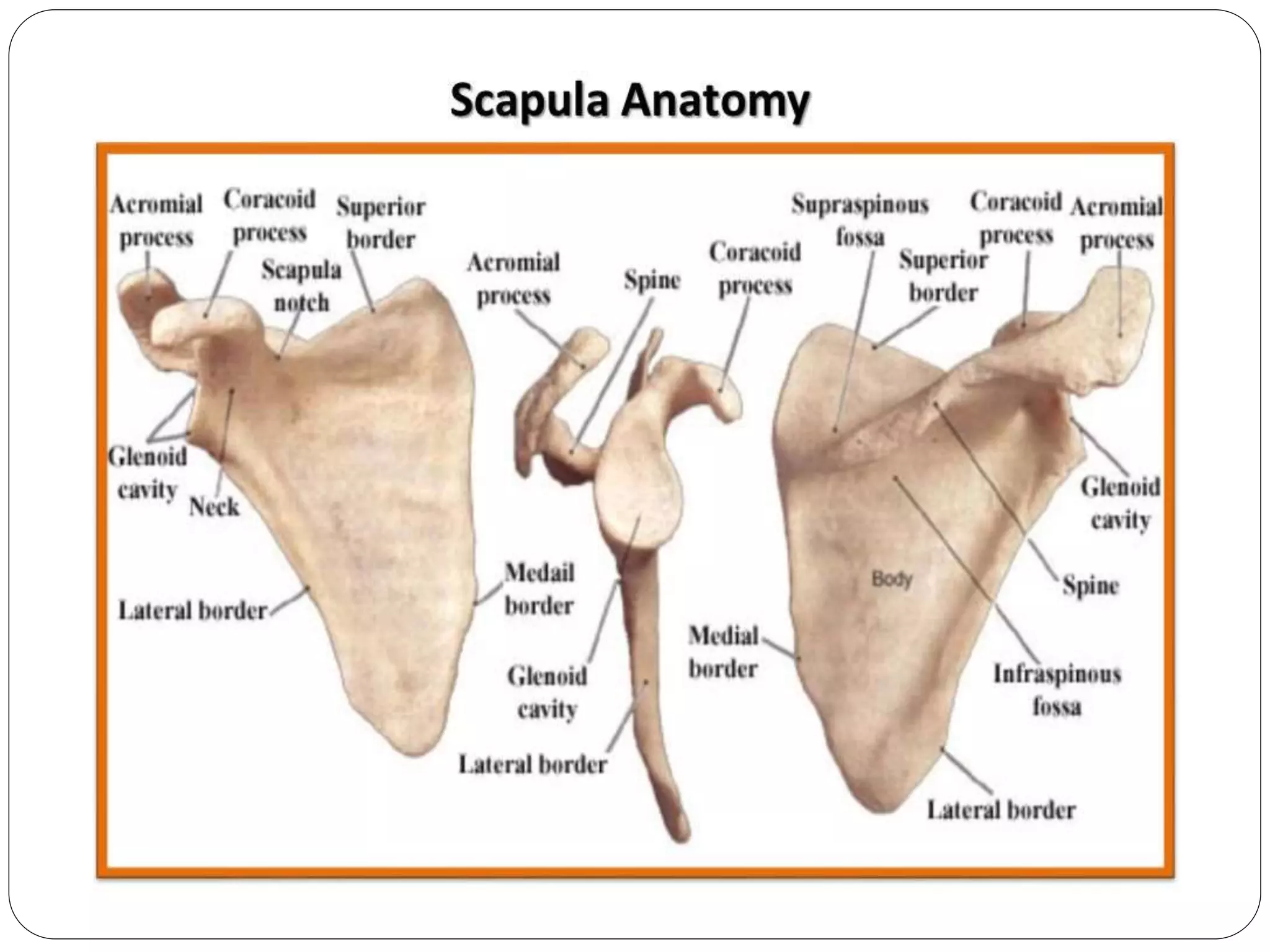
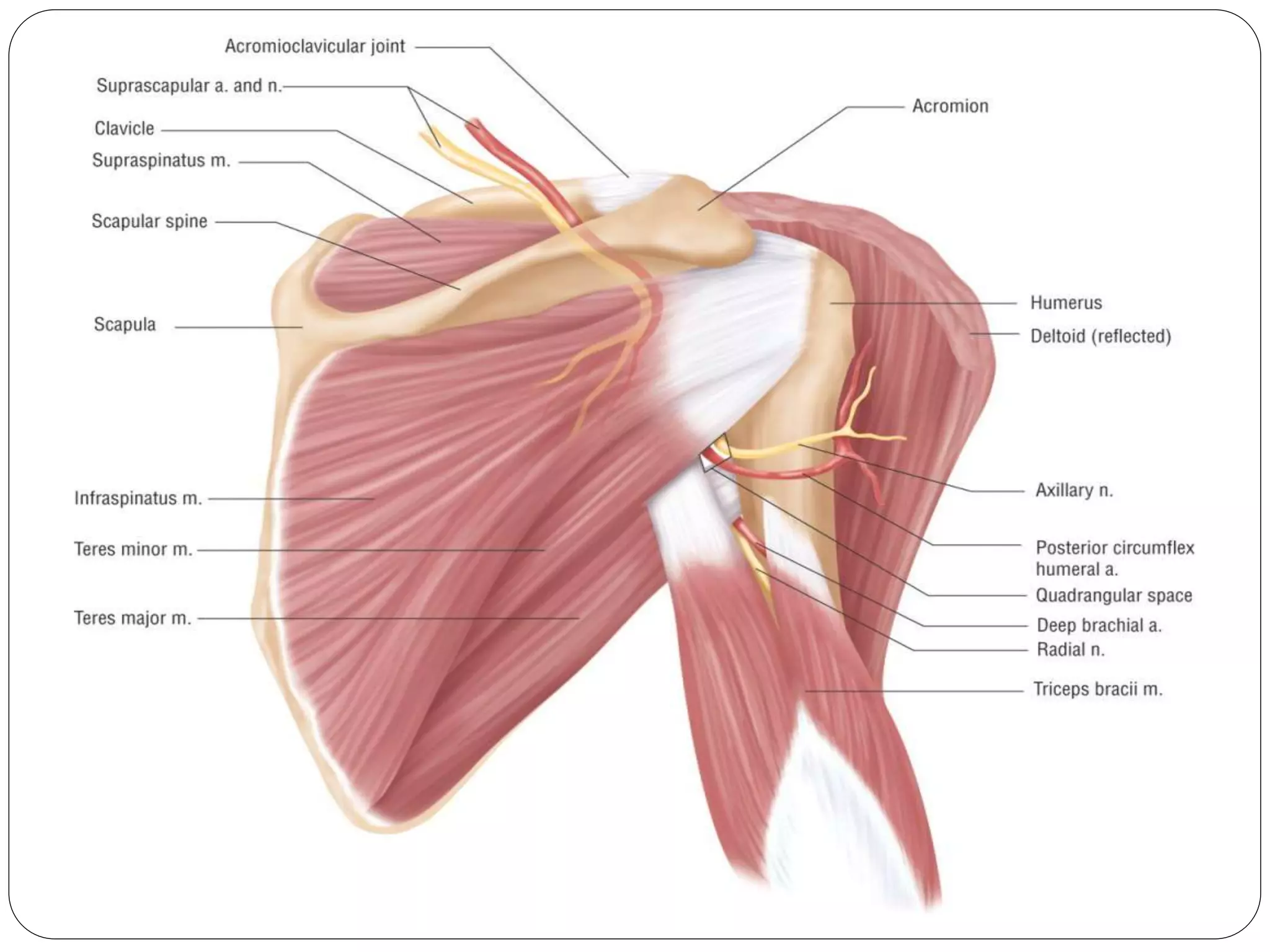
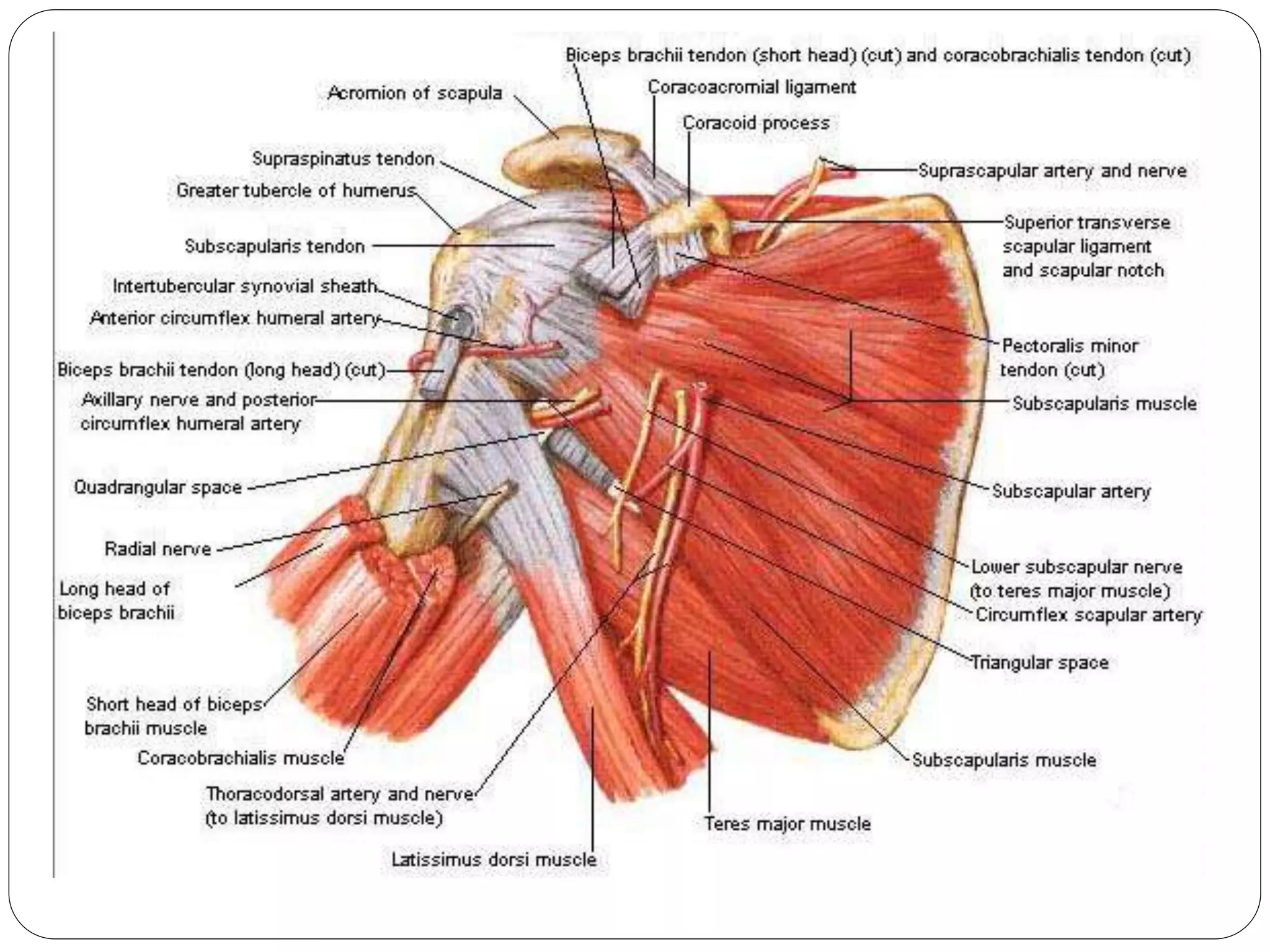
Basic anatomyand its surgical importance.
Mechanism of injury.
# incidence and associated injuries.
Diagnosis.
Classification
Treatment
Complication .
Recent literature.
12.
Mechanism of injury
Direct blunt trauma – most
common.
Indirect :
Traction injuries by pull of muscles
and ligaments around
induces avulsion injuries of
acromian and coracoid. Rarely
seen during seizures/electric
shock.
Humeral head impaction- glenoid /
13.
Mode of
injury:
Highenergy trauma: road
traffic accident- most
common.
Fall from height.
Crush injuries.
Sporting activities- boxing,
horse riding, skiing,contact
sport.
14.
Associated injuries
Verycommon- 61%-98%. More severe then
scapula fracture which may delay diagnosis and
treatment .
Chest injuries-ribs #-most common. 8-54%
Neurovasclar injuries- brachial plexus 5-13%
Head injuries.20%
Splenic and liver lacerations 3-5%.
Mortality due to associated injuries- 2-15%.
15.
Diagnosis
Clinical :pain, crepitus ,tenderness, painful
movements.
Echymosis is less than expected due to thick
muscular cover.
Pseudo rupture of rotator cuff: due to
intramuscular hematoma- resolves within week.
Examination must include evaluation of chest
,head and neurovascular structure.
Operative indication:
Glenoid #
IdebergI: >1 cm displacement,
25% ant rim,33% posterior rim #
with glenohumeral instability.
Tpe II,III,IV,V: > 5 mm
displacement.
Type VI: orif not indicated due
to extensive comminution.
25.
Scapula neck#
>1 cm translation.
> 40* angulation/ GPA< 20*
Associated displaced SSSC injury.
Scapula body:
non operative irrespective of no of
fragments.
heals with malunion.
26.
Complications:
With fracture:brachial plexus , supra
scapular,axillary nerve injury. Rotator cuff injury.
Conservative treatment: malunion, rarely non
union, stiffness, arthritis,instability,
Operative treatment: lantry 2008 injury
hardware removal 7 %
infection 4 %
nerve injury 2%
arhritis,rotator cuff dysfunction heterotrphic
ossification. Rarely non union
27.
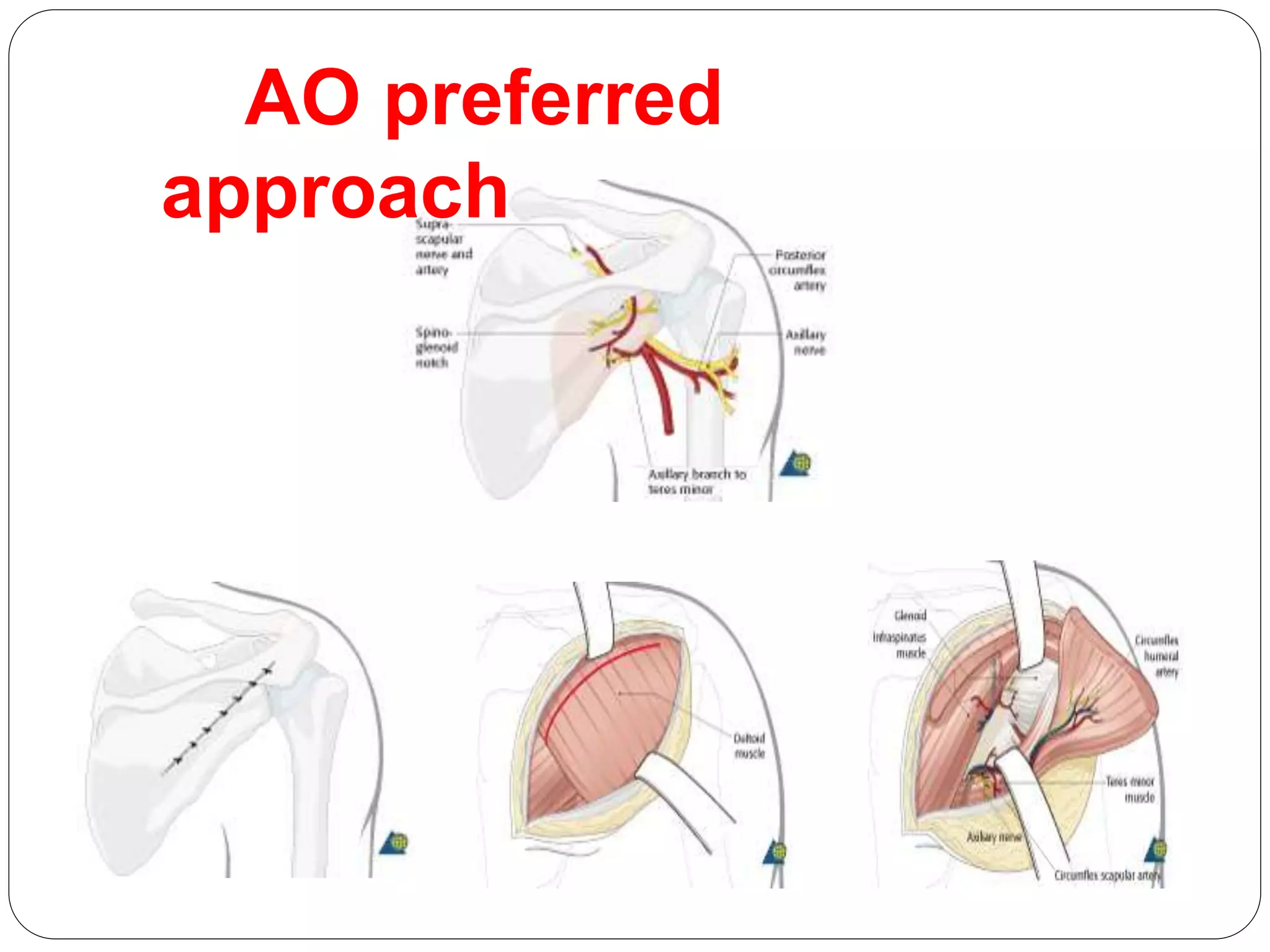
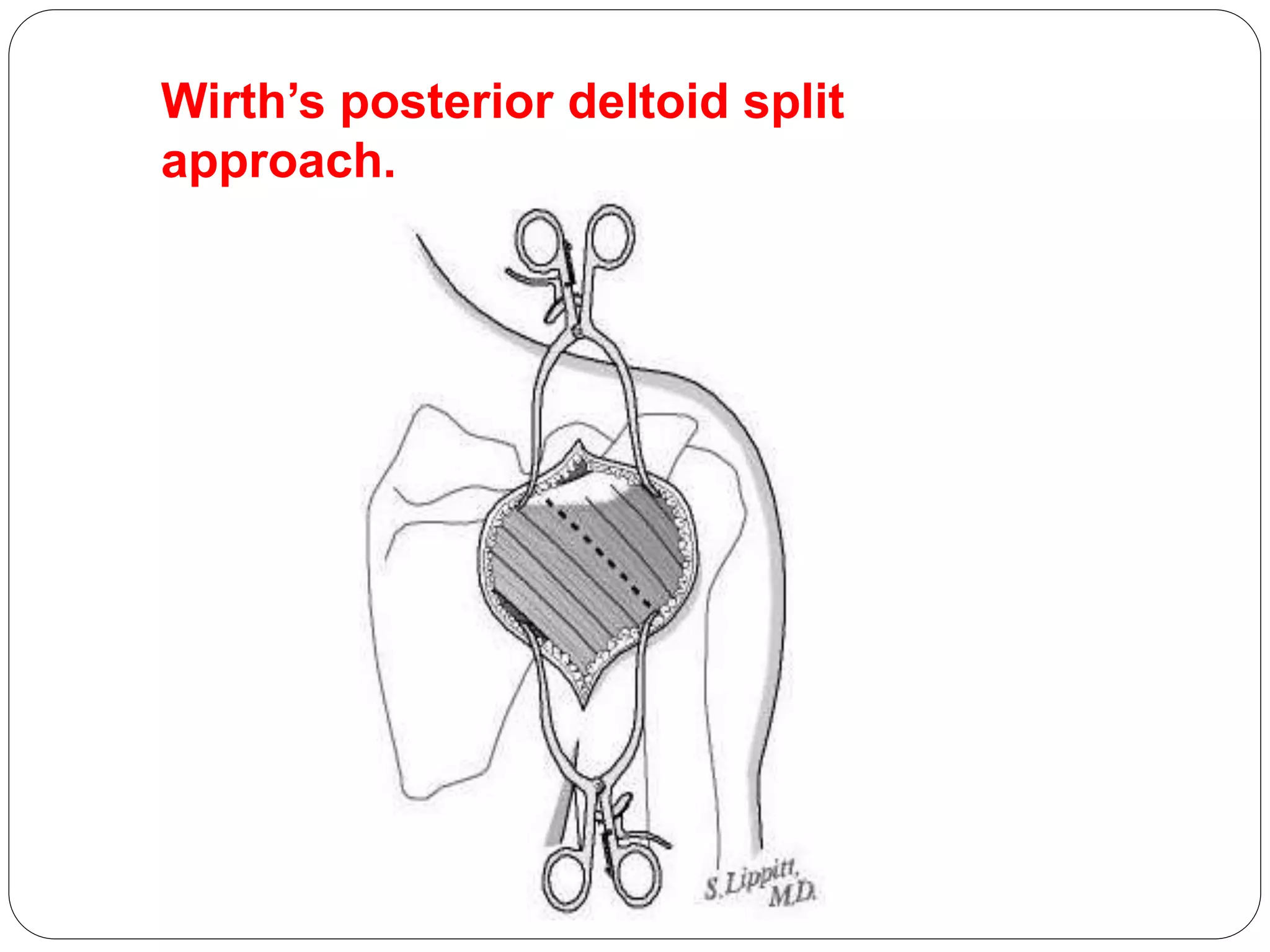
Surgical approaches.
Anterior– deltopectoral interval .
Superior - between spinous process and clavicle.
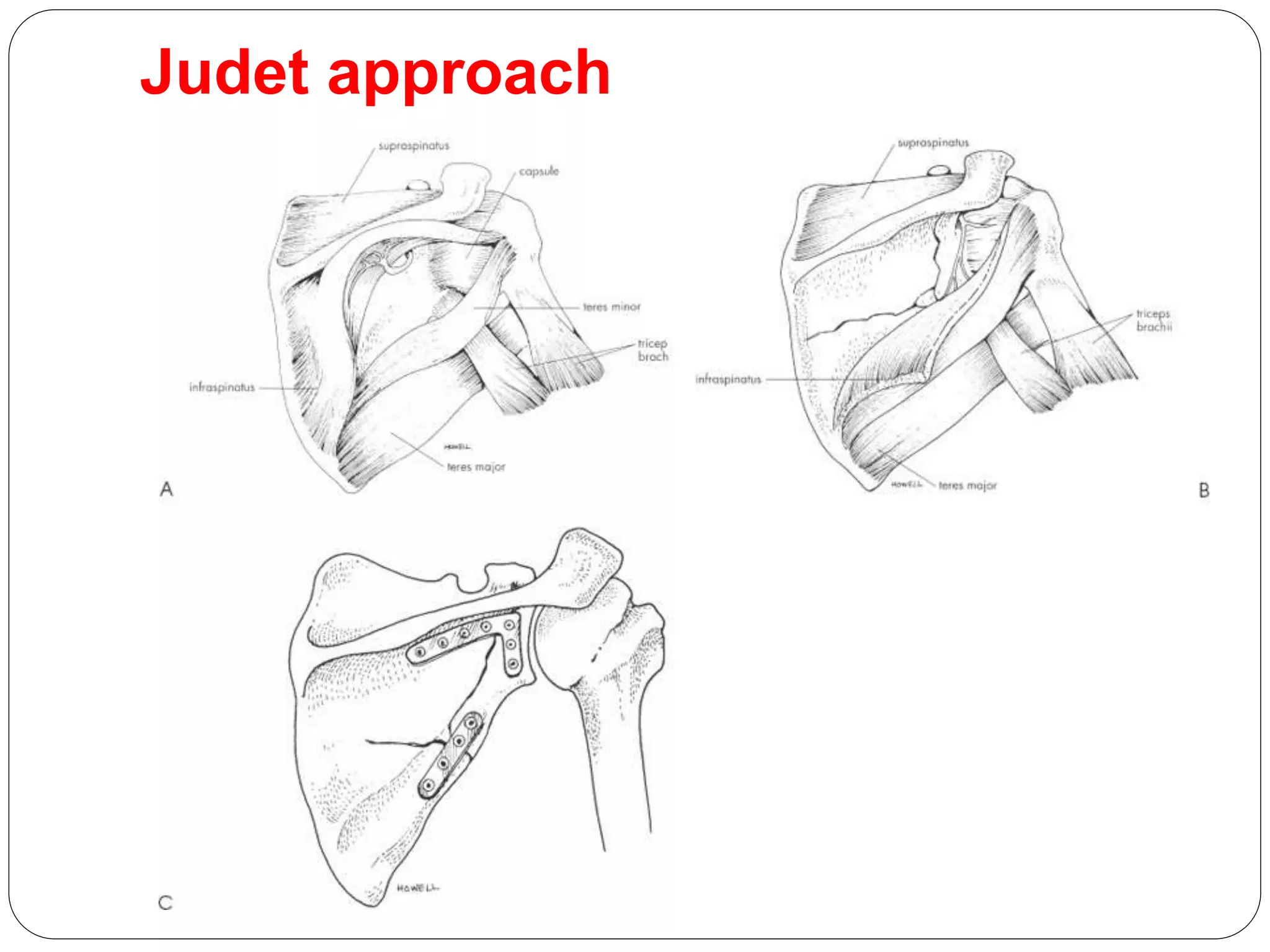
Posterior- classical judet approach.
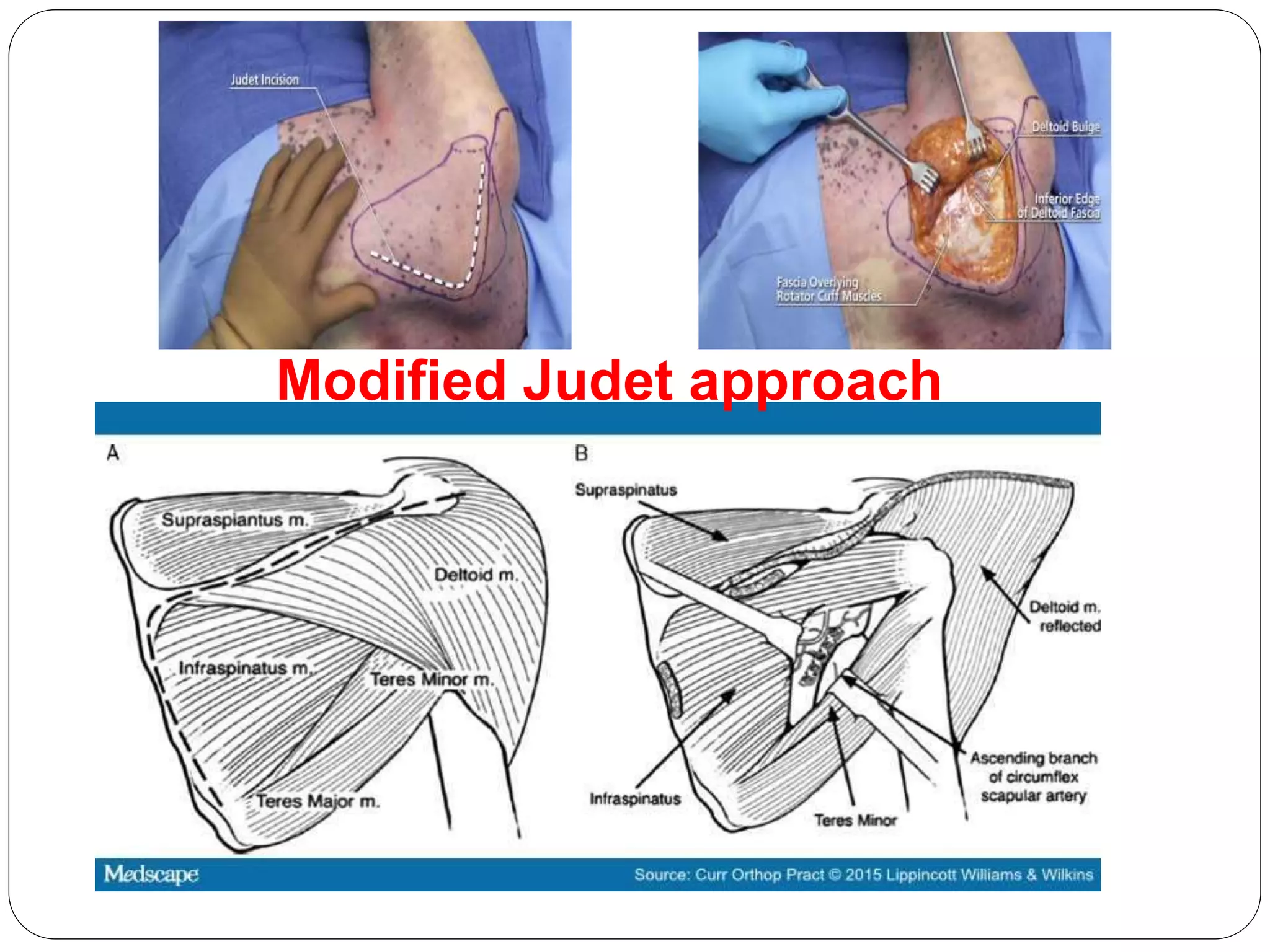
Modified judet approach.
Ebraheim’s reverse judet incision
approach.
Brodsky’s and Jerosch’s vertical
incision approach.
Surgical Exposure andFixation of Displaced Type
IV, V,
and VI Glenoid Fractures
Sean E. Nork, MD, David P. Barei, MD, Michael J. Gardner, MD, Thomas A.
Schildhauer, MD,
Keith A. Mayo, MD, and Stephen K. Benirschke, MD
J Orthop Trauma 2008;22:487–493
Both lateral and prone positioning may be used. Lateral
positioning allows access to the coracoid process for
manipulation of anterior or cephalad articular fracture
fragments. However, intraoperative fluoroscopic maging is
extremely difficult in this position.
Prone positioning has the advantage of facilitating
intraoperative fluoroscopic imaging, which may be helpful in
particularly difficult fracture patterns. However, prone
positioning has increased anesthetic risks and does not
allow access to the coracoid process.
42.
Operative treatment ofscapular fractures:
A systematic review
Jacob M. Lantry a, Craig S. Roberts a,*, Peter V. Giannoudis
Injury, Int. J. Care Injured (2008) 39, 271—283
The most common injuries treated with surgery were
glenoid fossa fractures and scapular neck fractures.
Approximately 25% of the cases had a concomitant
injury to the clavicle or acromioclavicular ligaments.
Internal fixation was most often achieved with a plate
and screws through a posterior approach.
The complication rate was low with infection, shoulder
stiffness, and implant failure the most commonly
reported problems.
Good to excellent functional results were obtained in
approximately 85% of the cases an average of 49.9
months postoperatively.
Take home message.
Always search for associated injuries.
Rule out chest trauma and neurological insult.
Whenever suspicion in CXR, get scapula trauma
series or CT done.
Avoid delayed diagnosis in Polytrauma patients.
Acceptable surgical indication:
Fracture displacement >20mm
Angulation >45*
GPA < 20*
Intra-articular step >4mm/>25% glenoid involved.
Displaced double disruption of SSSC.
45.
Delayed treatment.>3 weeks still give favorable
results.
Preferred implant : 3.5 mm recon locking plate/
tubular plates and ccs.
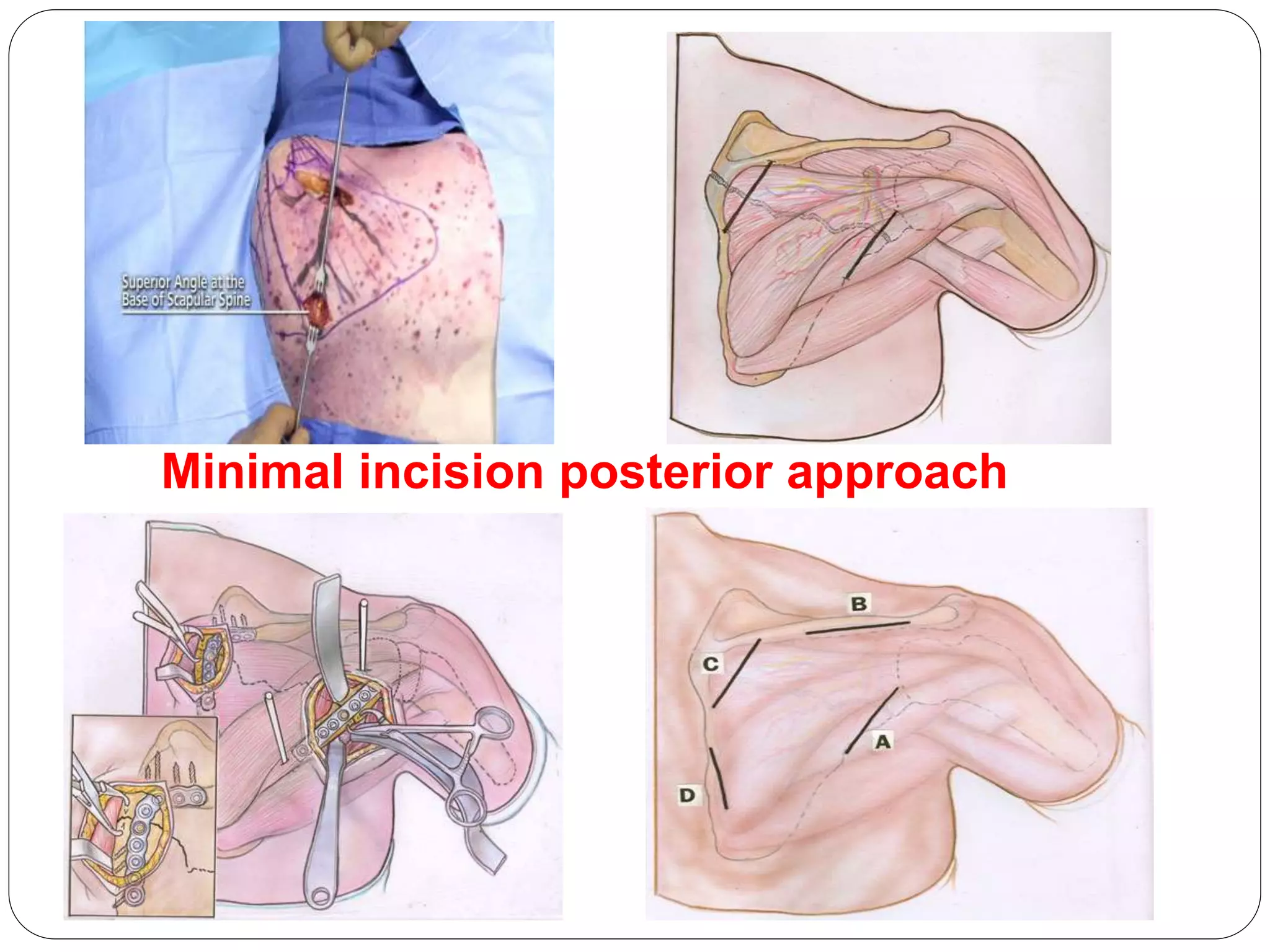
Preferred approach: posterior minimal v/s
modified judet depending on fracture pattern and
extend.
Avoid intra op injury to neurovascluar structure.
Post op complication less.
Avoid rotator cuff injury and stiffness.