Posterolateral corner injuries of knee joint Samir Dwidmuthe
Missed posterolateral corner injuries of knee joint is a common cause for failure of ACL and PCL reconstruction only next to malpositioned tunnels.
Isolated PLC injuries are uncommon, making up <2% of all acute knee ligamentous injuries. Covey JBJS 2001
Incidence of PLC injuries associated with concomitant ACL and PCL disruptions are much more common (43% to 80%). Ranawat JAAOS 2008
A recent (MRI) analysis of surgical tibialplateau fractures demonstrated an incidence of PLC injuries in 68% of cases. Gardner JOT 2005
Take home message
PLC injuries to be ruled out in every case of ACL& PCL rupture.
Neurovascular integrity to be checked in every case.
Grade I & II can be managed conservatively.
Grade III Acute- Repair.
Grade III Chronic- Anatomic PLC recon.
Beware of varus knee alignment.
Posterolateral corner injuries of knee joint Samir Dwidmuthe
Missed posterolateral corner injuries of knee joint is a common cause for failure of ACL and PCL reconstruction only next to malpositioned tunnels.
Isolated PLC injuries are uncommon, making up <2% of all acute knee ligamentous injuries. Covey JBJS 2001
Incidence of PLC injuries associated with concomitant ACL and PCL disruptions are much more common (43% to 80%). Ranawat JAAOS 2008
A recent (MRI) analysis of surgical tibialplateau fractures demonstrated an incidence of PLC injuries in 68% of cases. Gardner JOT 2005
Take home message
PLC injuries to be ruled out in every case of ACL& PCL rupture.
Neurovascular integrity to be checked in every case.
Grade I & II can be managed conservatively.
Grade III Acute- Repair.
Grade III Chronic- Anatomic PLC recon.
Beware of varus knee alignment.
a summary of the pertinent elbow anatomy, mechanism of injury, primary and secondary stabilizers of the elbow, and treatment options of elbow terrible triad
a summary of the pertinent elbow anatomy, mechanism of injury, primary and secondary stabilizers of the elbow, and treatment options of elbow terrible triad
These simplified slides by Dr. Sidra Arshad present an overview of the non-respiratory functions of the respiratory tract.
Learning objectives:
1. Enlist the non-respiratory functions of the respiratory tract
2. Briefly explain how these functions are carried out
3. Discuss the significance of dead space
4. Differentiate between minute ventilation and alveolar ventilation
5. Describe the cough and sneeze reflexes
Study Resources:
1. Chapter 39, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 34, Ganong’s Review of Medical Physiology, 26th edition
3. Chapter 17, Human Physiology by Lauralee Sherwood, 9th edition
4. Non-respiratory functions of the lungs https://academic.oup.com/bjaed/article/13/3/98/278874
Pulmonary Thromboembolism - etilogy, types, medical- Surgical and nursing man...VarunMahajani
Disruption of blood supply to lung alveoli due to blockage of one or more pulmonary blood vessels is called as Pulmonary thromboembolism. In this presentation we will discuss its causes, types and its management in depth.
Tom Selleck Health: A Comprehensive Look at the Iconic Actor’s Wellness Journeygreendigital
Tom Selleck, an enduring figure in Hollywood. has captivated audiences for decades with his rugged charm, iconic moustache. and memorable roles in television and film. From his breakout role as Thomas Magnum in Magnum P.I. to his current portrayal of Frank Reagan in Blue Bloods. Selleck's career has spanned over 50 years. But beyond his professional achievements. fans have often been curious about Tom Selleck Health. especially as he has aged in the public eye.
Follow us on: Pinterest
Introduction
Many have been interested in Tom Selleck health. not only because of his enduring presence on screen but also because of the challenges. and lifestyle choices he has faced and made over the years. This article delves into the various aspects of Tom Selleck health. exploring his fitness regimen, diet, mental health. and the challenges he has encountered as he ages. We'll look at how he maintains his well-being. the health issues he has faced, and his approach to ageing .
Early Life and Career
Childhood and Athletic Beginnings
Tom Selleck was born on January 29, 1945, in Detroit, Michigan, and grew up in Sherman Oaks, California. From an early age, he was involved in sports, particularly basketball. which played a significant role in his physical development. His athletic pursuits continued into college. where he attended the University of Southern California (USC) on a basketball scholarship. This early involvement in sports laid a strong foundation for his physical health and disciplined lifestyle.
Transition to Acting
Selleck's transition from an athlete to an actor came with its physical demands. His first significant role in "Magnum P.I." required him to perform various stunts and maintain a fit appearance. This role, which he played from 1980 to 1988. necessitated a rigorous fitness routine to meet the show's demands. setting the stage for his long-term commitment to health and wellness.
Fitness Regimen
Workout Routine
Tom Selleck health and fitness regimen has evolved. adapting to his changing roles and age. During his "Magnum, P.I." days. Selleck's workouts were intense and focused on building and maintaining muscle mass. His routine included weightlifting, cardiovascular exercises. and specific training for the stunts he performed on the show.
Selleck adjusted his fitness routine as he aged to suit his body's needs. Today, his workouts focus on maintaining flexibility, strength, and cardiovascular health. He incorporates low-impact exercises such as swimming, walking, and light weightlifting. This balanced approach helps him stay fit without putting undue strain on his joints and muscles.
Importance of Flexibility and Mobility
In recent years, Selleck has emphasized the importance of flexibility and mobility in his fitness regimen. Understanding the natural decline in muscle mass and joint flexibility with age. he includes stretching and yoga in his routine. These practices help prevent injuries, improve posture, and maintain mobilit
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stockrebeccabio
Factory Supply Best Quality Pmk Oil CAS 28578–16–7 PMK Powder in Stock
Telegram: bmksupplier
signal: +85264872720
threema: TUD4A6YC
You can contact me on Telegram or Threema
Communicate promptly and reply
Free of customs clearance, Double Clearance 100% pass delivery to USA, Canada, Spain, Germany, Netherland, Poland, Italy, Sweden, UK, Czech Republic, Australia, Mexico, Russia, Ukraine, Kazakhstan.Door to door service
Hot Selling Organic intermediates
The prostate is an exocrine gland of the male mammalian reproductive system
It is a walnut-sized gland that forms part of the male reproductive system and is located in front of the rectum and just below the urinary bladder
Function is to store and secrete a clear, slightly alkaline fluid that constitutes 10-30% of the volume of the seminal fluid that along with the spermatozoa, constitutes semen
A healthy human prostate measures (4cm-vertical, by 3cm-horizontal, 2cm ant-post ).
It surrounds the urethra just below the urinary bladder. It has anterior, median, posterior and two lateral lobes
It’s work is regulated by androgens which are responsible for male sex characteristics
Generalised disease of the prostate due to hormonal derangement which leads to non malignant enlargement of the gland (increase in the number of epithelial cells and stromal tissue)to cause compression of the urethra leading to symptoms (LUTS
These lecture slides, by Dr Sidra Arshad, offer a quick overview of physiological basis of a normal electrocardiogram.
Learning objectives:
1. Define an electrocardiogram (ECG) and electrocardiography
2. Describe how dipoles generated by the heart produce the waveforms of the ECG
3. Describe the components of a normal electrocardiogram of a typical bipolar leads (limb II)
4. Differentiate between intervals and segments
5. Enlist some common indications for obtaining an ECG
Study Resources:
1. Chapter 11, Guyton and Hall Textbook of Medical Physiology, 14th edition
2. Chapter 9, Human Physiology - From Cells to Systems, Lauralee Sherwood, 9th edition
3. Chapter 29, Ganong’s Review of Medical Physiology, 26th edition
4. Electrocardiogram, StatPearls - https://www.ncbi.nlm.nih.gov/books/NBK549803/
5. ECG in Medical Practice by ABM Abdullah, 4th edition
6. ECG Basics, http://www.nataliescasebook.com/tag/e-c-g-basics
Ozempic: Preoperative Management of Patients on GLP-1 Receptor Agonists Saeid Safari
Preoperative Management of Patients on GLP-1 Receptor Agonists like Ozempic and Semiglutide
ASA GUIDELINE
NYSORA Guideline
2 Case Reports of Gastric Ultrasound
ARTIFICIAL INTELLIGENCE IN HEALTHCARE.pdfAnujkumaranit
Artificial intelligence (AI) refers to the simulation of human intelligence processes by machines, especially computer systems. It encompasses tasks such as learning, reasoning, problem-solving, perception, and language understanding. AI technologies are revolutionizing various fields, from healthcare to finance, by enabling machines to perform tasks that typically require human intelligence.
Title: Sense of Taste
Presenter: Dr. Faiza, Assistant Professor of Physiology
Qualifications:
MBBS (Best Graduate, AIMC Lahore)
FCPS Physiology
ICMT, CHPE, DHPE (STMU)
MPH (GC University, Faisalabad)
MBA (Virtual University of Pakistan)
Learning Objectives:
Describe the structure and function of taste buds.
Describe the relationship between the taste threshold and taste index of common substances.
Explain the chemical basis and signal transduction of taste perception for each type of primary taste sensation.
Recognize different abnormalities of taste perception and their causes.
Key Topics:
Significance of Taste Sensation:
Differentiation between pleasant and harmful food
Influence on behavior
Selection of food based on metabolic needs
Receptors of Taste:
Taste buds on the tongue
Influence of sense of smell, texture of food, and pain stimulation (e.g., by pepper)
Primary and Secondary Taste Sensations:
Primary taste sensations: Sweet, Sour, Salty, Bitter, Umami
Chemical basis and signal transduction mechanisms for each taste
Taste Threshold and Index:
Taste threshold values for Sweet (sucrose), Salty (NaCl), Sour (HCl), and Bitter (Quinine)
Taste index relationship: Inversely proportional to taste threshold
Taste Blindness:
Inability to taste certain substances, particularly thiourea compounds
Example: Phenylthiocarbamide
Structure and Function of Taste Buds:
Composition: Epithelial cells, Sustentacular/Supporting cells, Taste cells, Basal cells
Features: Taste pores, Taste hairs/microvilli, and Taste nerve fibers
Location of Taste Buds:
Found in papillae of the tongue (Fungiform, Circumvallate, Foliate)
Also present on the palate, tonsillar pillars, epiglottis, and proximal esophagus
Mechanism of Taste Stimulation:
Interaction of taste substances with receptors on microvilli
Signal transduction pathways for Umami, Sweet, Bitter, Sour, and Salty tastes
Taste Sensitivity and Adaptation:
Decrease in sensitivity with age
Rapid adaptation of taste sensation
Role of Saliva in Taste:
Dissolution of tastants to reach receptors
Washing away the stimulus
Taste Preferences and Aversions:
Mechanisms behind taste preference and aversion
Influence of receptors and neural pathways
Impact of Sensory Nerve Damage:
Degeneration of taste buds if the sensory nerve fiber is cut
Abnormalities of Taste Detection:
Conditions: Ageusia, Hypogeusia, Dysgeusia (parageusia)
Causes: Nerve damage, neurological disorders, infections, poor oral hygiene, adverse drug effects, deficiencies, aging, tobacco use, altered neurotransmitter levels
Neurotransmitters and Taste Threshold:
Effects of serotonin (5-HT) and norepinephrine (NE) on taste sensitivity
Supertasters:
25% of the population with heightened sensitivity to taste, especially bitterness
Increased number of fungiform papillae
micro teaching on communication m.sc nursing.pdfAnurag Sharma
Microteaching is a unique model of practice teaching. It is a viable instrument for the. desired change in the teaching behavior or the behavior potential which, in specified types of real. classroom situations, tends to facilitate the achievement of specified types of objectives.
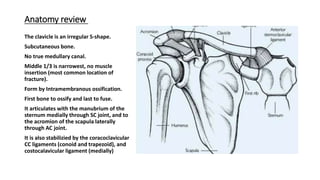
1. Anatomy review
The clavicle is an irregular S-shape.
Subcutaneous bone.
No true medullary canal.
Middle 1/3 is narrowest, no muscle
insertion (most common location of
fracture).
Form by Intramembranous ossification.
First bone to ossify and last to fuse.
It articulates with the manubrium of the
sternum medially through SC joint, and to
the acromion of the scapula laterally
through AC joint.
It is also stabilizied by the coracoclavicular
CC ligaments (conoid and trapezoid), and
costocalavicular ligament (medially)
6. Group I (Middle third) 80%
Non-Displaced :-
Less than 100% displacement
Non-operative
displaced :-
Greater than 100% displacement
Nonunion rate of 4.5%
operative
9. Type II displaced 2ndry to
a fracture line medial to
the CC ligament
Type II A :-
conoid and trapezoid
attached (fracture medial to
CC ligaments)
Medial clavicle unstable
Up to 56% nonunion rate with
nonoperative management
Operative
10. Type II B :-
conoid torn, trapezoid attached (fracture
between the CC ligaments)
Medial clavicle unstable
Up to 30-45% nonunion rate with
nonoperative management
Operative
11. Type III
fracture of the articular surface
Conoid and trapezoid intact therefore stable
injury
Non-operative
12. Type IV
periosteal sleeve fracture (children)
Conoid and trapezoid ligaments remain
attached to periosteum and overall the
fracture pattern is stable
Non-operative
17. deformity forces on
clavicular fracture
•the sternocleidomastoid
muscle pulls the medial
fragment posterosuperiorly
•pectoralis and weight of
arm pull the lateral
fragment inferomedially
18. Diagnosis
plain X-ray:-
• standard AP view of bilateral shoulders to measure clavicular
shortening
• 15° cephalic tilt (ZANCA view) determine superior/inferior
displacement
CT scan
• may help evaluate displacement, shortening, comminution, articular
extension, and nonunion
• useful for medial physeal fractures and sternoclavicular injuries
19.
20. Treatment
Non-operative
sling immobilization with gentle
ROM exercises at 2-4 weeks and
strengthening at 6-10 weeks.
Operative
• Closed Reduction,
Intramedullary Fixation
• Open Reduction, Plate and
Screw Fixation
21. Indications:
• minimally displaced.
• shortening and displacement <2cm
• no neurologic deficit
Indications:
absolute
• open fxs
• displaced fracture with skin tenting
• subclavian artery or vein injury
• floating shoulder (clavicle and scapula neck fx)
• symptomatic nonunion
• symptomatic malunion
• unstable fracture patterns (Type IIA, Type IIB, Type
V)
relative and controversial indications
• displaced Group I (middle third) with >2cm
shortening
• bilateral, displaced clavicle fractures
• brachial plexus injury (questionable b/c 66% have
spontaneous return)
• closed head injury
• seizure disorder
• polytrauma patient
22.
23. Close reduction and intramedullary fixation
(titanium elastic nail)
Advantage:-
1. Small incision and less soft tissue disruption
2. Less prominent
3. Avoid supraclavicular cutaneous nerve injury
Disadvantage:-
1. Hardware migration
2. Biomechanically inferior to plating
24.
25.
26.
27. Open Reduction, Plate and Screw Fixation
Superior of anteroinferior plating
Hook plate
43. 4-neurovascular injury
superior plates associated with increased risk of subclavian artery or vein penetration.
5-pneumothorax.
6-non-union.
7-adhesive capsulitis.
45. Anatomy
• AC joint is a synovial joint with a fibrocartilaginous disk.
• It has thin capsule that is stabilized by sup. Inf. Ant. and post.
Ligaments.
• superior and posterior ligaments are most important.
• Vertical stability is provided by the CC ligaments:-
• Trapezoid insert 3cm from end of clavicle.
• Conoid insert 4,5cm from end of clavicle.
• Normal AC joint are 5 to 6 mm in width.
• Normal CC distance is 1,1 cm to 1,3 cm.
46.
47. Mechanism of injury
• Fall on shoulder or
direct blow to the
acromion with arm
adducted. (most
common)
• Fall on outstretched
arm transmitted to AC
joint.
• Rugby and hockey
players frequently
sustained this injury.
50. Type 2
A.C joint and capsule are
disrupted.
C.C ligaments are intact.
Less than or equal to 50%
vertical subluxation of the
clavicle.
The C.C interval is slightly
increase (<25%).
reducible.
51. Type 3
Rupture of both ACJ and
CC ligaments.
Complete loss of contact
between clavicle and
acromion.
CC interval is increased
from 25-100%.
Reducible.
52. Type 4
Rupture of ACJ and CC
ligaments with
displacement of clavicle
posteriorly through
trapezoid.
not reducible.
53. Type 5
Rupture of both ACJ and
CC ligaments with gross
displacement of the ACJ
and detachment of
deltoid and trapezius.
not reducible.
55. • Symptoms
pain
• Physical exam
palpate for lateral clavicle or AC joint tenderness.
observe for abnormal contour of the shoulder compared to
contralateral side.
prominence of the distal calvicle
56.
57. Imaging
• bilateral AP view (compare displacement to contralateral side).
• 15 cephalic tilt (zanca view) to evaluate joint displacement and intra-
articular fracture.
• Axillary view is mandatory to determine AP displacement
58.
59.
60.
61.
62. Treatment:-
Non-operative:-
ice, rest and sling for 3 weeks.
regain functional motion by 6 weeks.
return to normal activity at 12 weeks.
• Indication:-
type 1, 2, and type 3 if displacement less than 2cm.
63. Operative:-
Indication:-
• Type 4, 5, 6
• Type 3 in athletes, and those with cosmetic concern.
rehabilitation
• sling immobilization without abduction for 6 weeks
• no shoulder ROM for 6 weeks
• generally return to full activity after 6 months
64. ORIF with Bosworth CC
screw fixation
Advantage:
Provide rigid fixation.
Disadvantage
1. Hardware irritation
2. Hardware failure
3. routine screw removal at 8-12wk is
advised to prevent screw breakage
65. ORIF with CC suture
fixation
Advantage:-
ORIF with CC suture fixation.
Disadvantage:-
• suture not as stronger as screw fixation.
• suture erosion causing distal third clavicle
fracture.
66. ORIF with hook plate
Advantage:-
rigid fixation
Disadvantage:-
acromial erosion.
hook pullout.
require second surgery for plate
removal.
69. CC ligament reconstruction
with free tendon graft
Advantage:-
graft reconstruction more closely
recreates strength of native CC
ligament
70. Complications:-
1. Residual pain at AC joint in 30-50%
2. AC arthritis:- more common with surgical management than with
nonop.
3. CC screw breakage/pullout