The document discusses anatomy, mechanism of injury, classification, diagnosis, and management of anterior shoulder dislocations. Key points include:
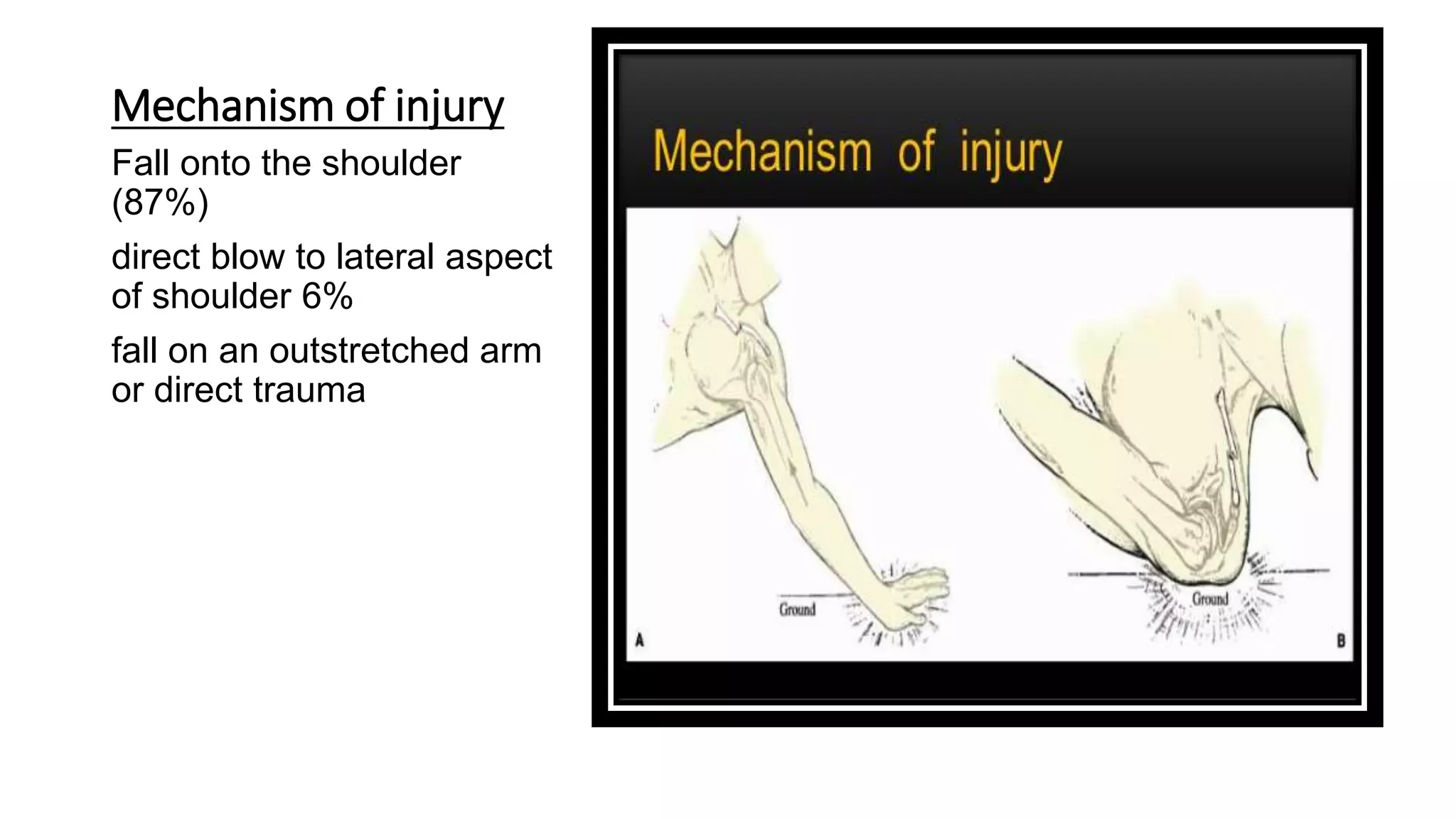
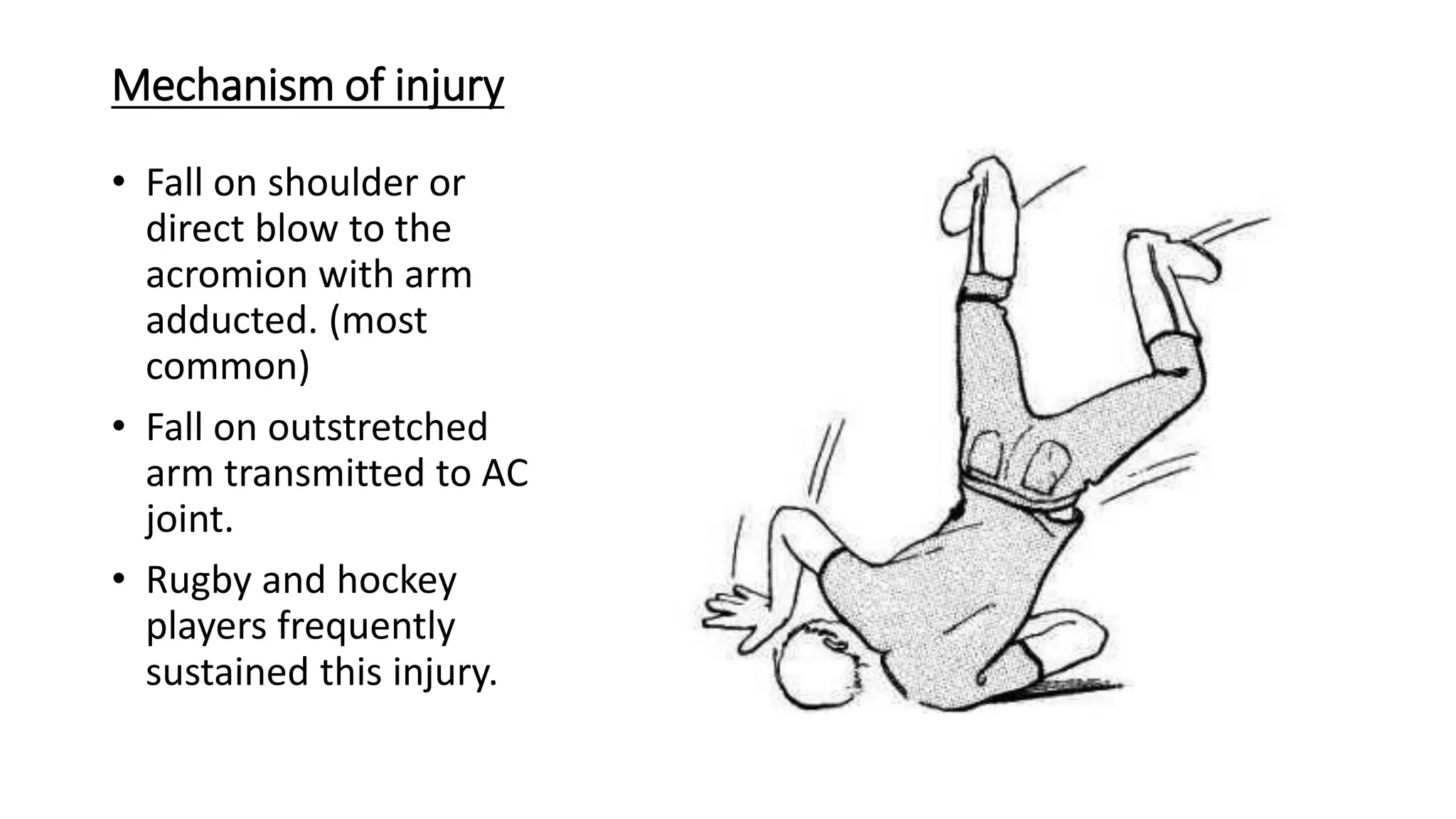
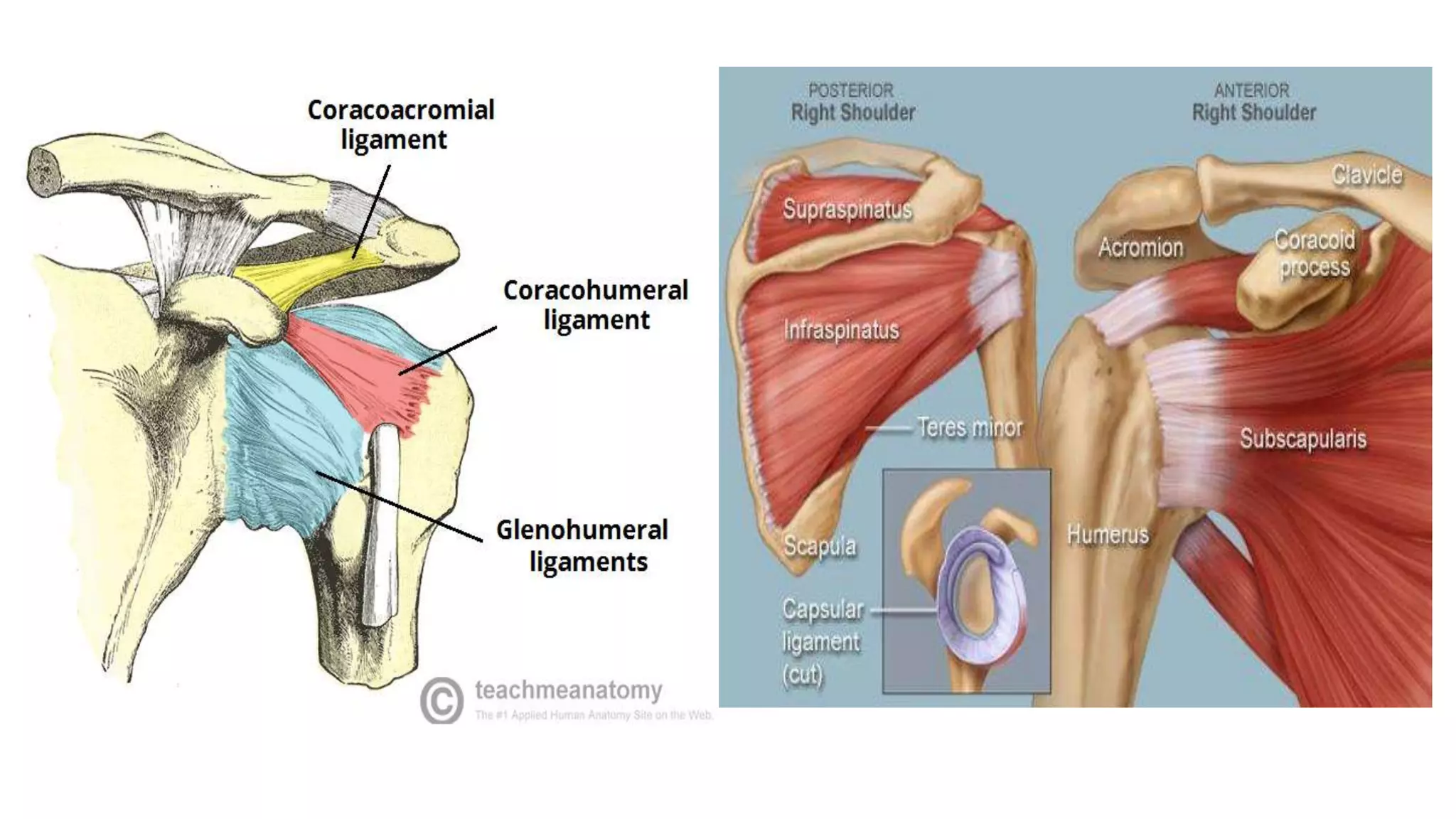
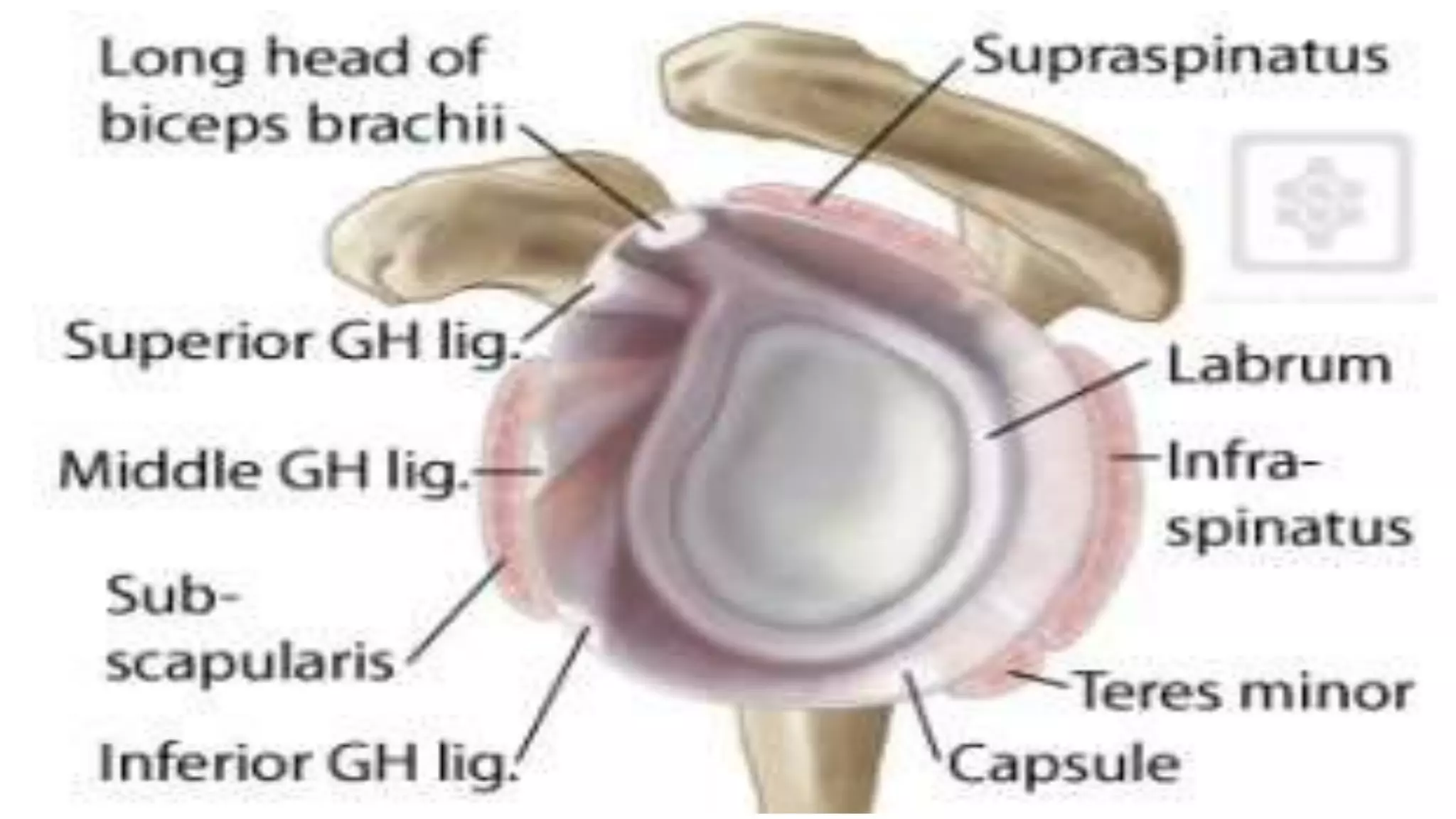
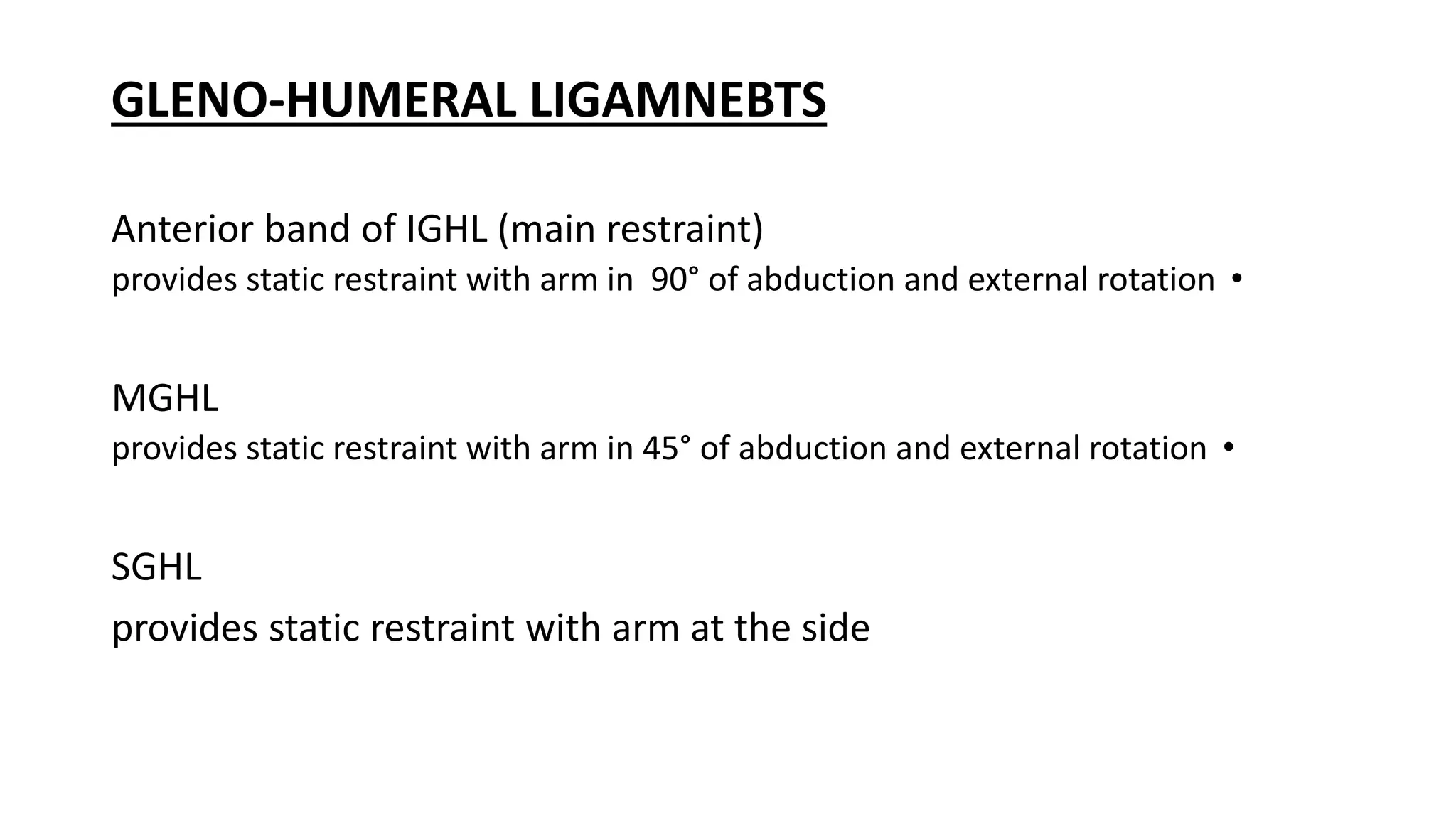
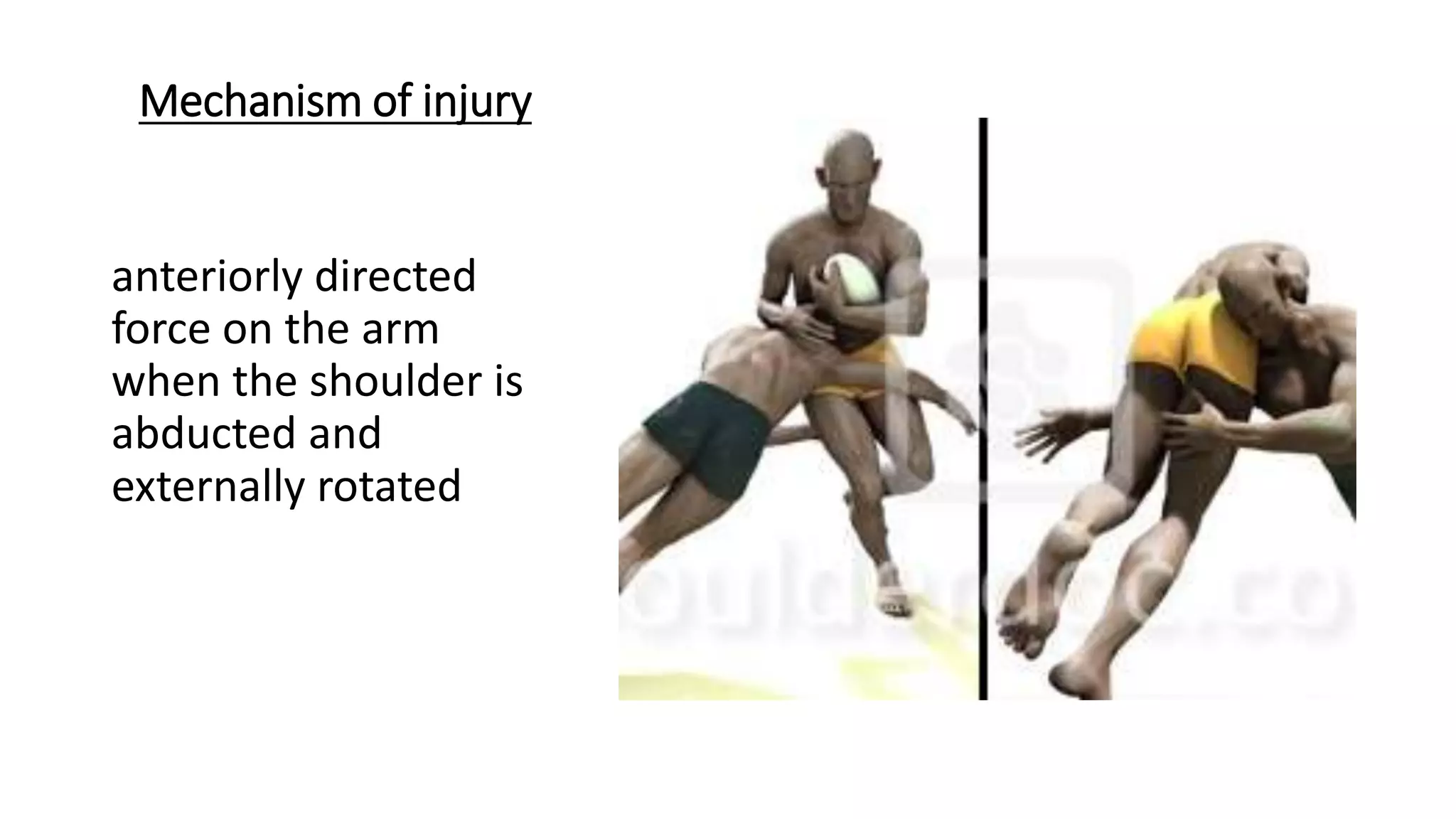
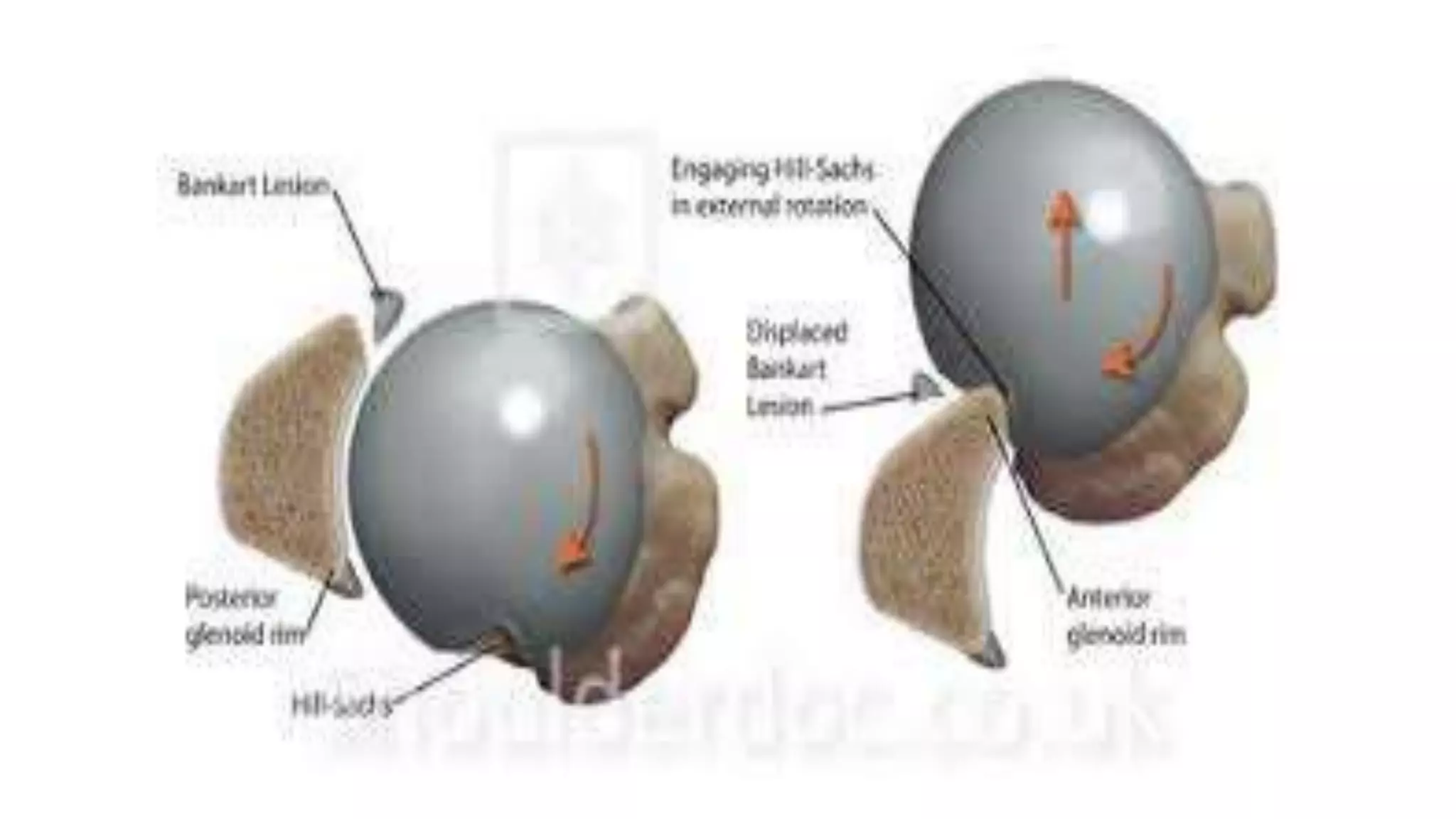
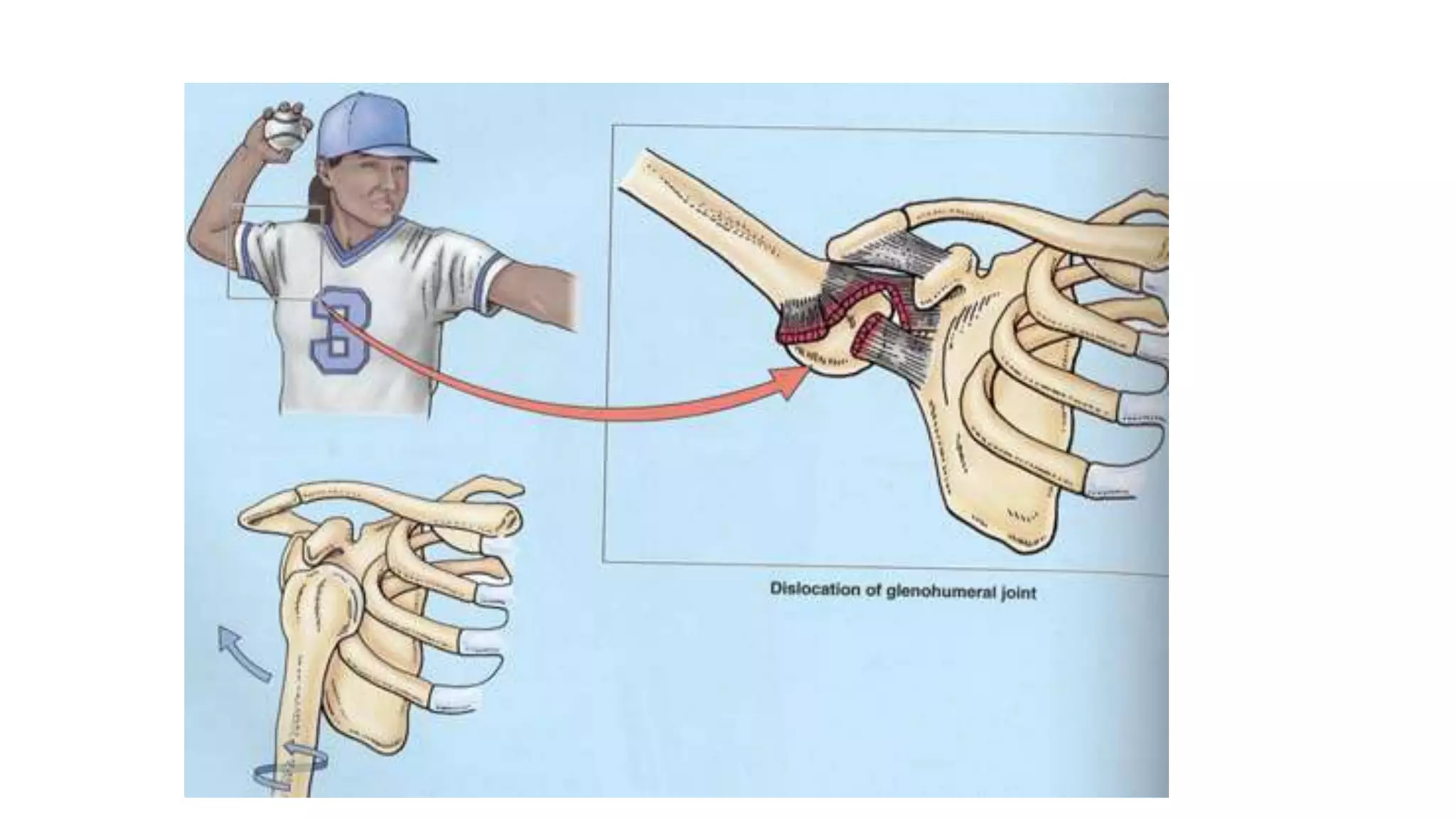
- Anterior shoulder dislocations are caused by an anteriorly directed force on the arm when abducted and externally rotated, which can tear the anterior labrum and ligaments.
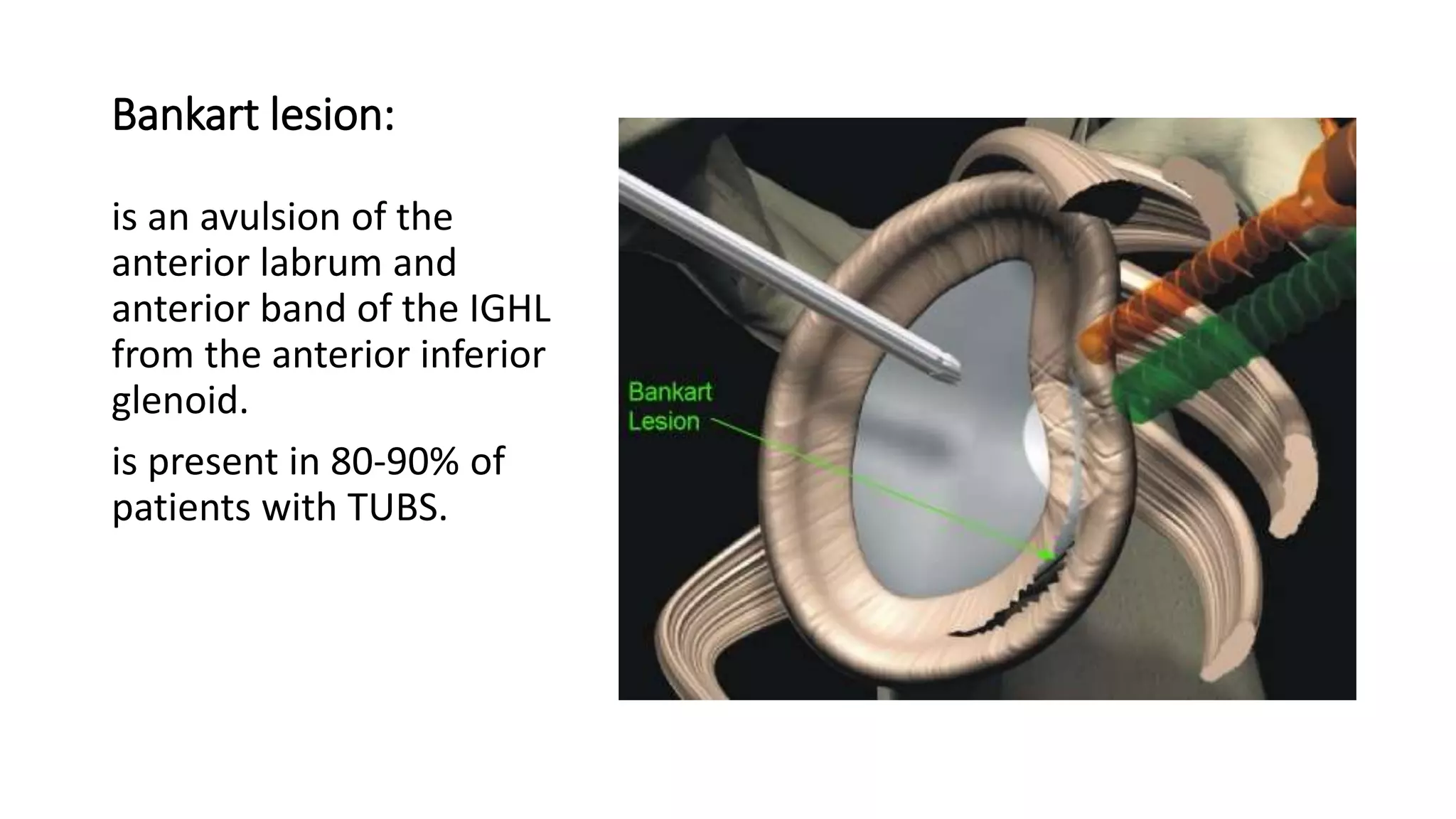
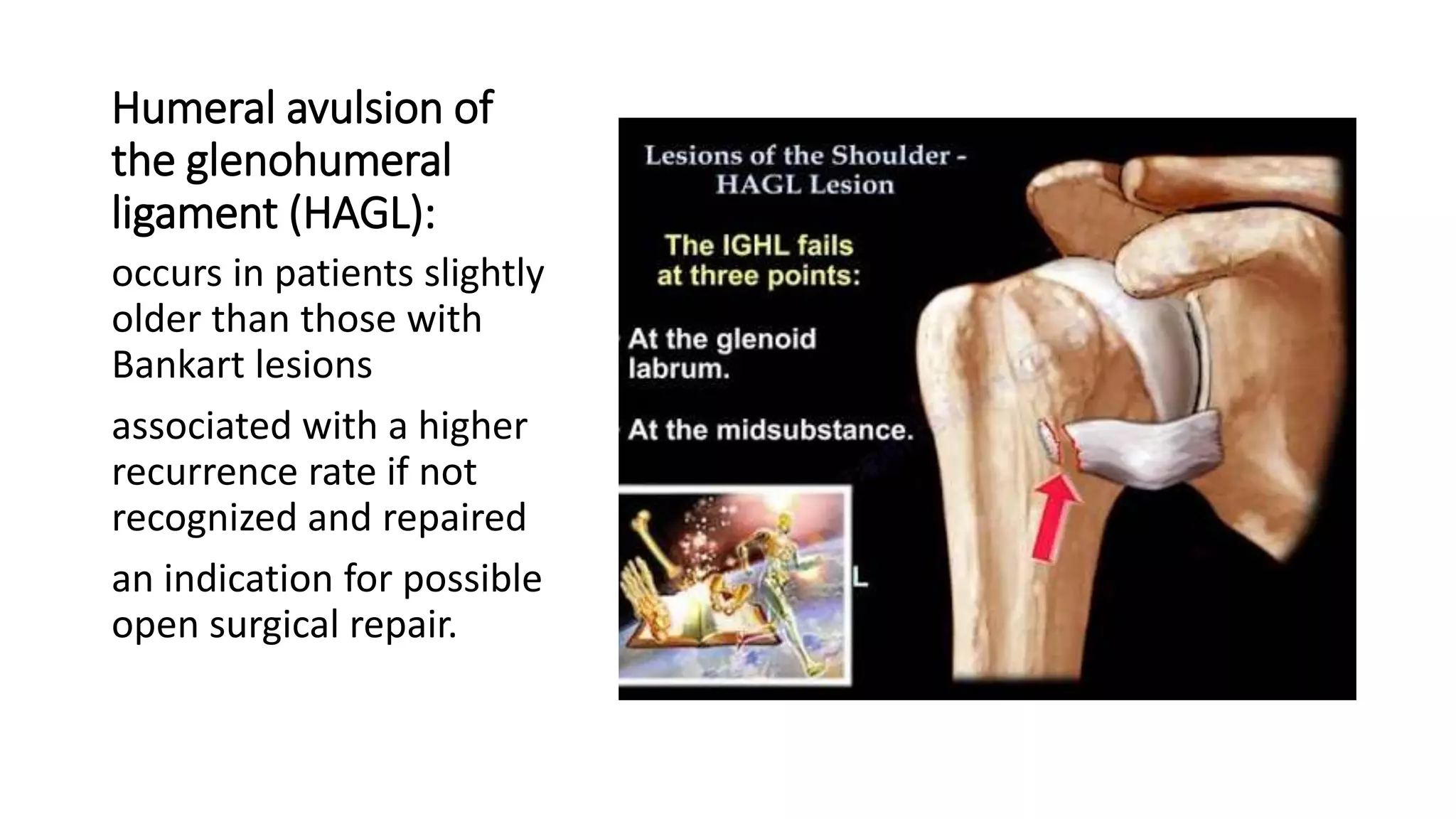
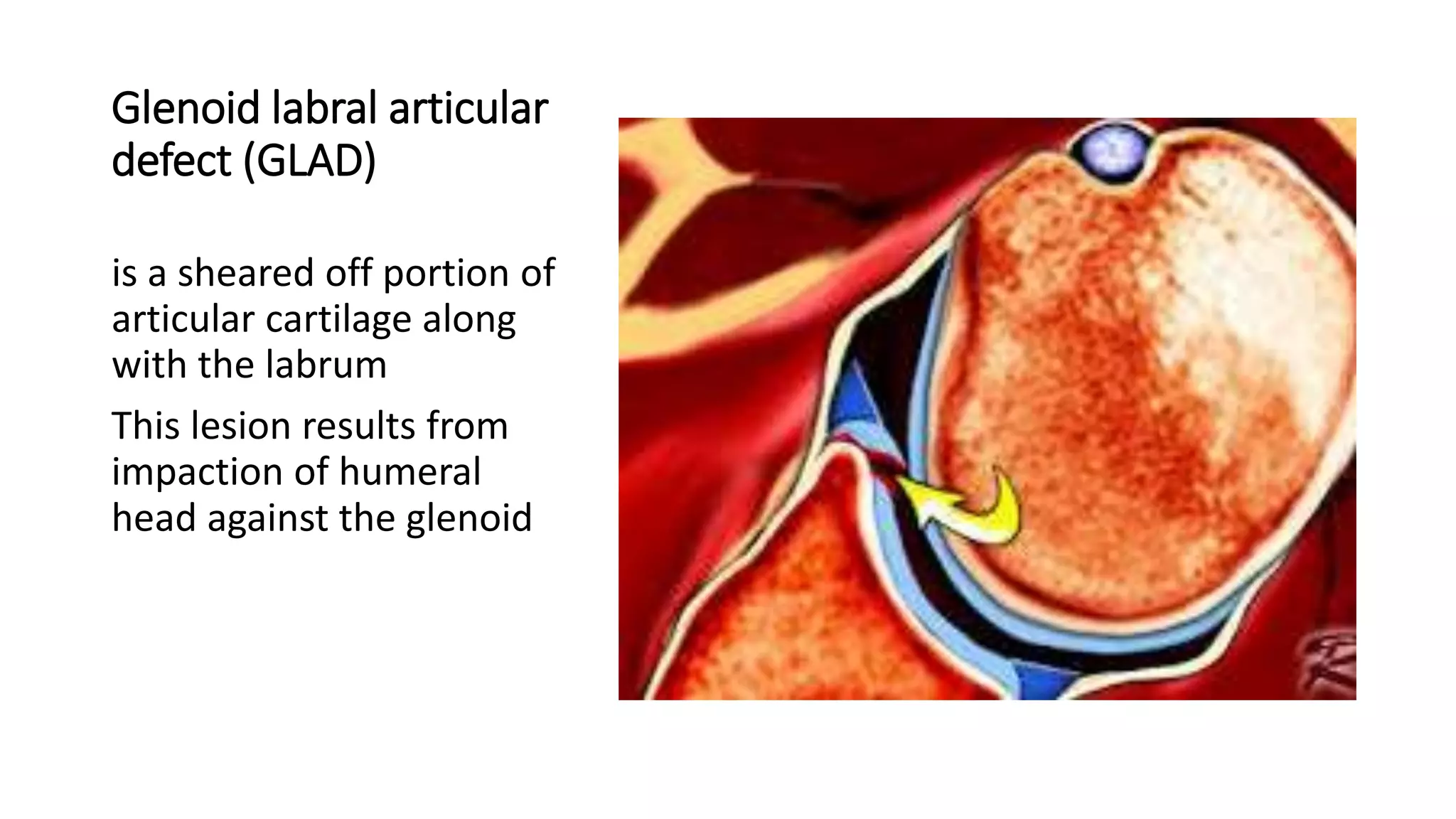
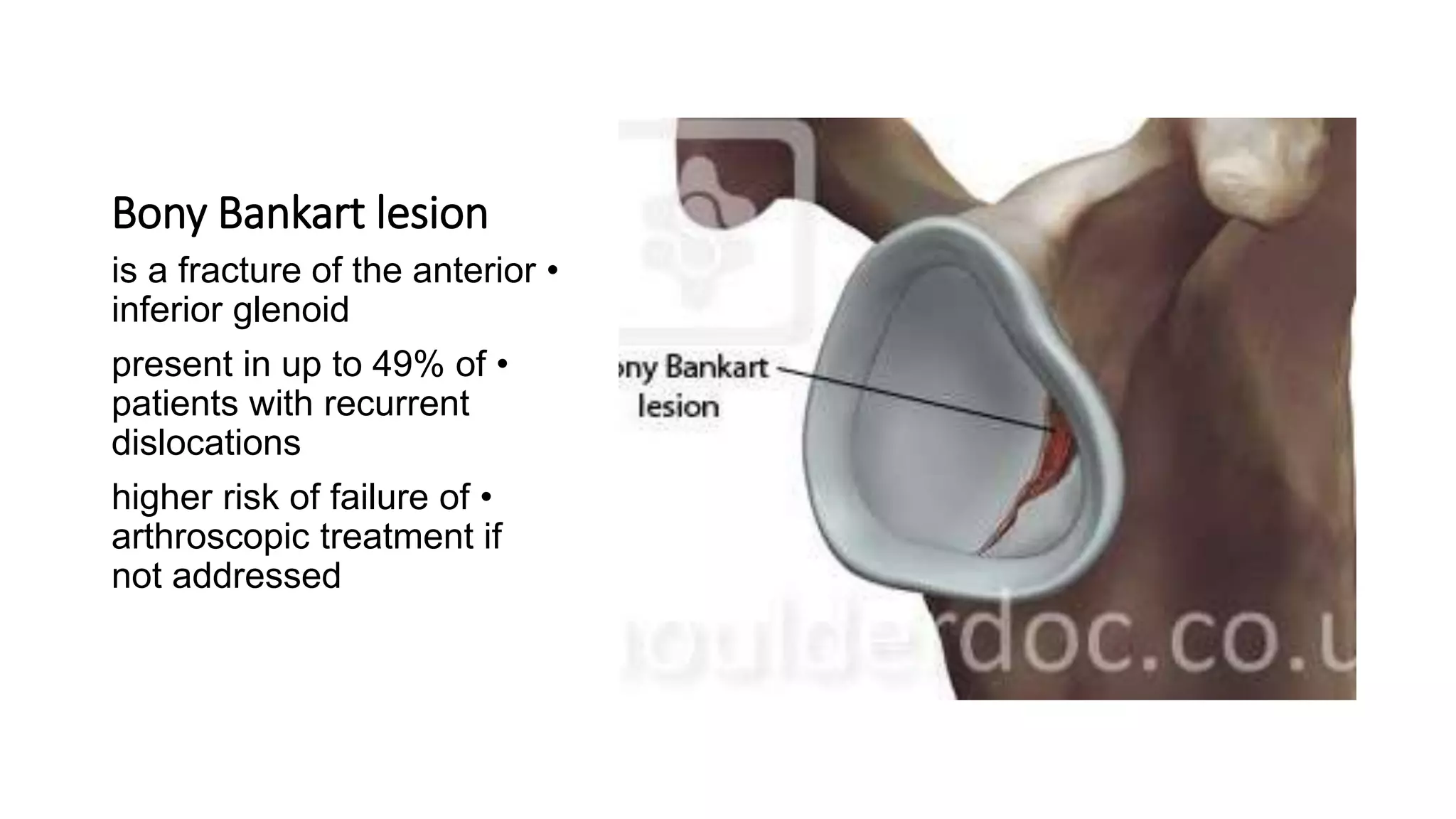
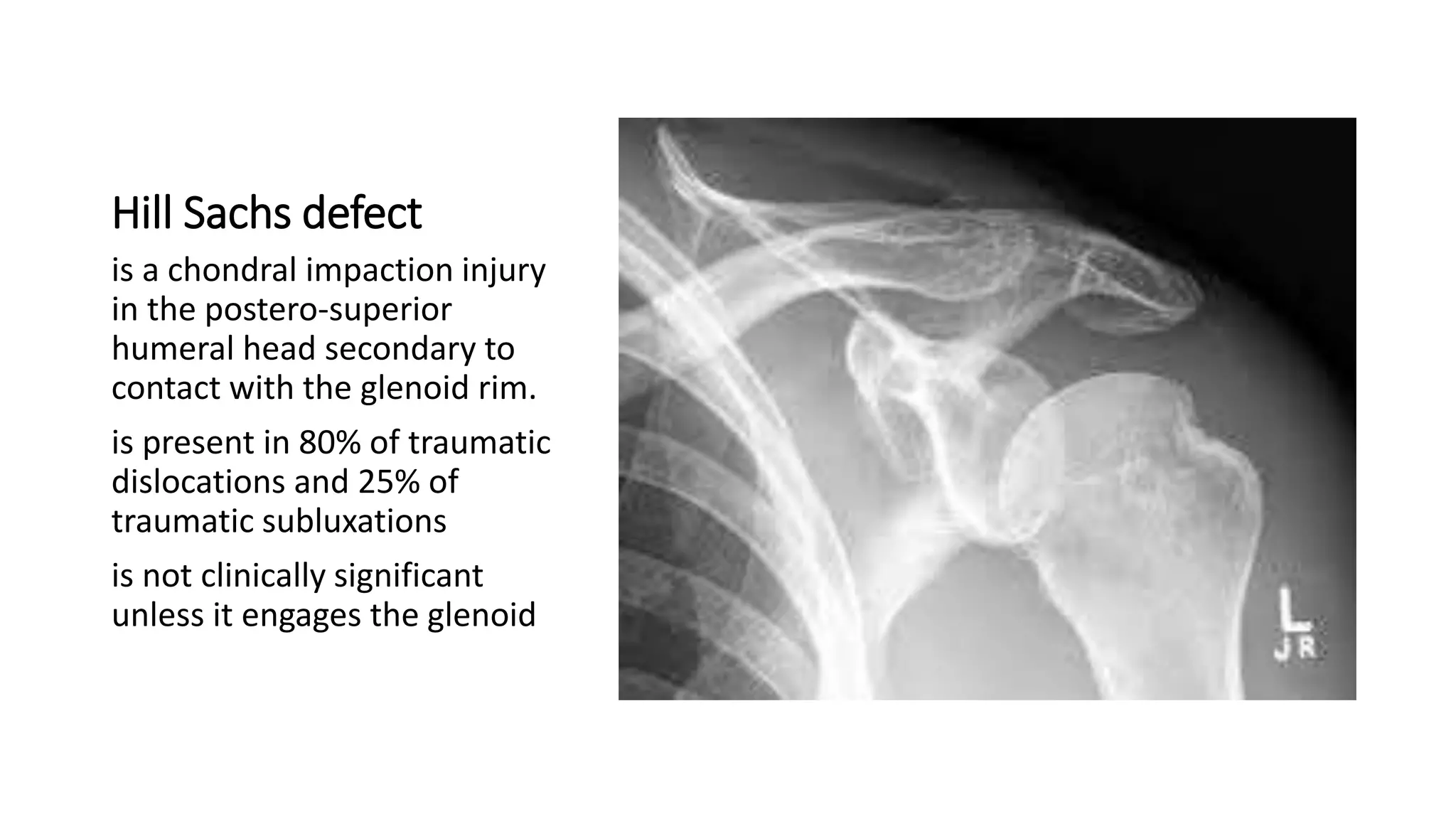
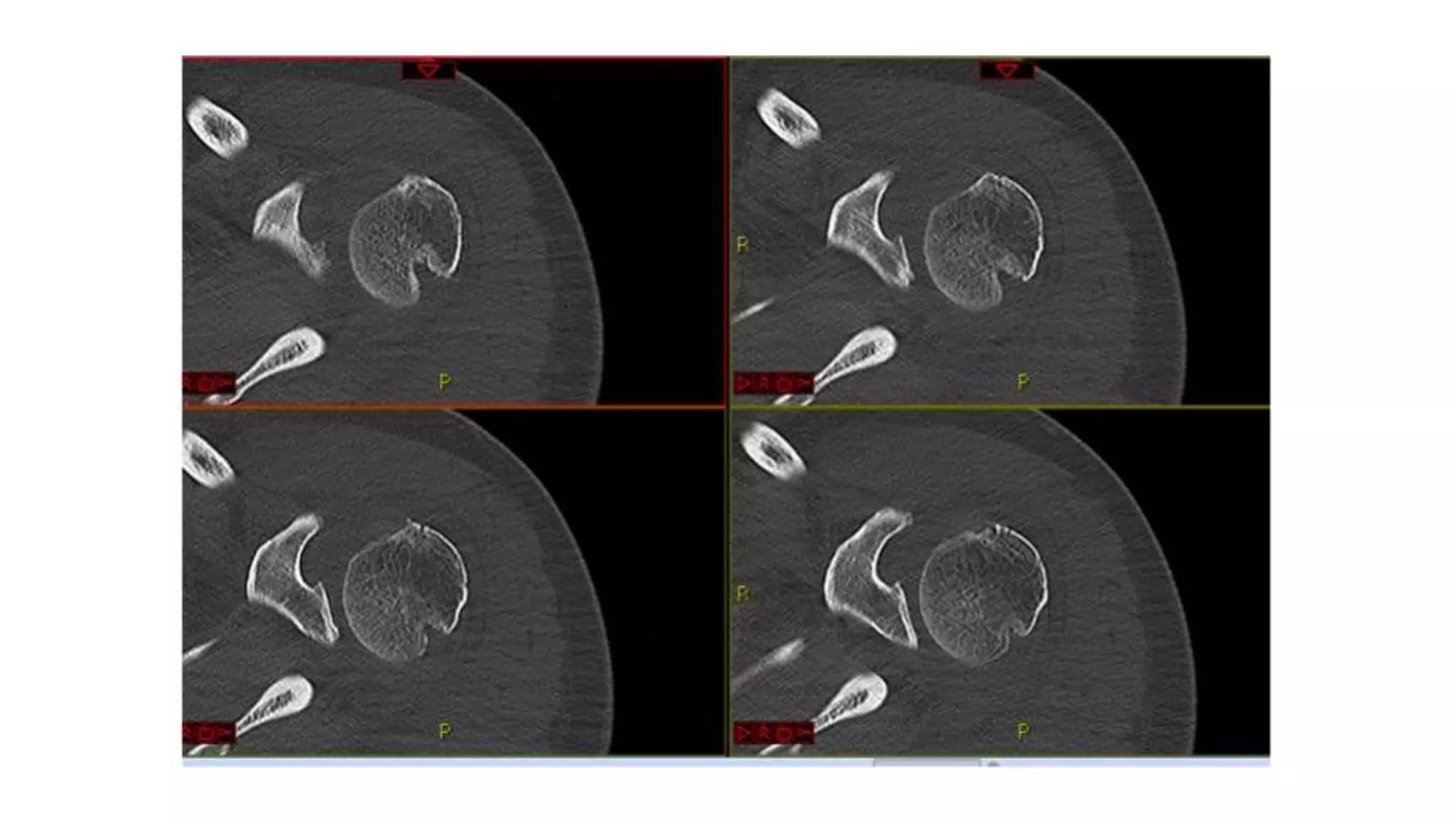
- Associated injuries may include bone fractures like bony Bankart lesions or Hill-Sachs defects. Labral injuries include Bankart lesions in 80-90% of cases.
- Treatment depends on any associated injuries and classification. Most cases are treated non-operatively with sling immobilization followed by physical therapy. Surgery is required for repair of labral tears or bone defects.