Downloaded 459 times
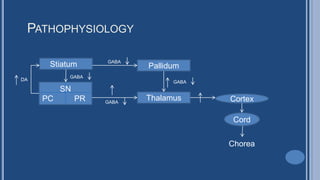
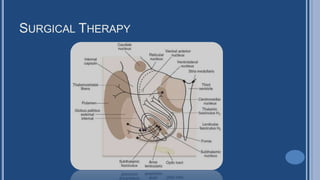
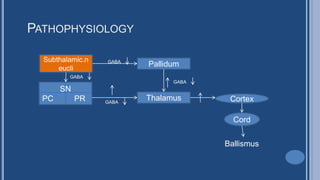



1. Chorea is a state of excessive, spontaneous, irregular movements that are randomly distributed and abnormal in character. It can range from mild restlessness to violent disabling movements. 2. Ballismus involves proximal, flinging, violent involuntary movements. Both chorea and ballismus are associated with basal ganglia dysfunction and abnormal neurotransmitter levels like decreased GABA and increased dopamine. 3. Causes of chorea and ballismus include infections, metabolic and endocrine disorders, drugs, trauma, vascular events, tumors, and hereditary conditions like Huntington's disease. Treatment involves reducing dopamine levels with antipsychotics or GABA agonists, as well as surgical procedures like pallidotomy or thalamotomy





























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)













