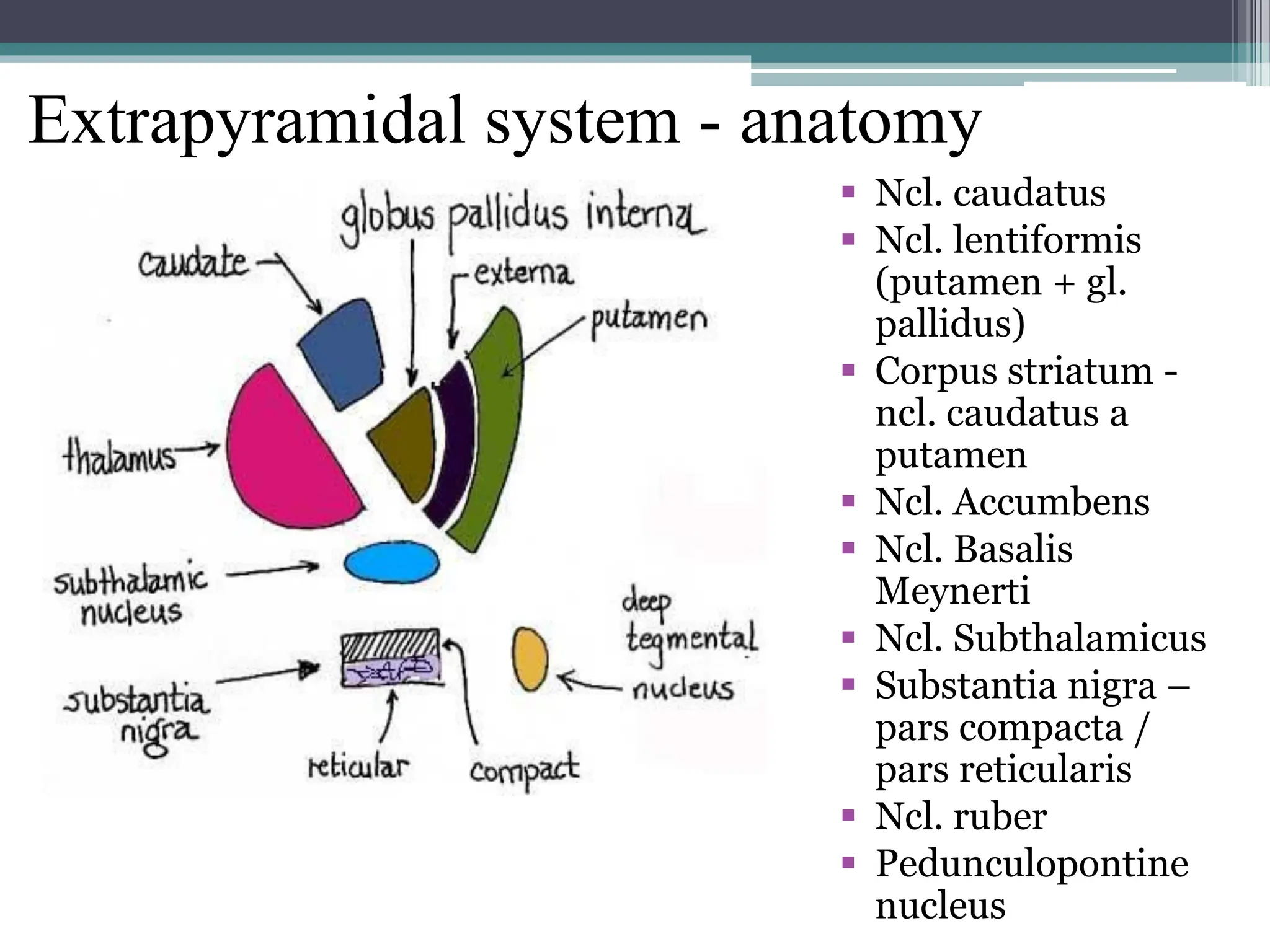
The document summarizes the anatomy and clinical features of the extrapyramidal system and cerebellum. It describes the anatomy of the extrapyramidal system including basal ganglia nuclei. It discusses extrapyramidal syndromes including hypokinetic syndromes like Parkinson's disease and hyperkinetic syndromes such as tremors, chorea, dystonia, and myoclonus. It also summarizes the anatomy of the cerebellum and clinical signs of cerebellar dysfunction including ataxia, tremor, and ocular motor abnormalities.