Downloaded 343 times

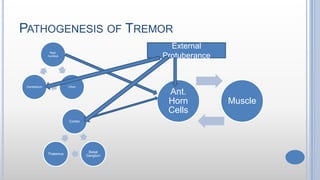



This document provides information on different types of tremors, including their causes, characteristics, and pathophysiology. It discusses rest tremor seen in Parkinson's disease and other conditions. It also covers postural tremor, physiological tremor, essential tremor, kinetic tremor, and cerebellar intention tremor. For each type of tremor, the summary highlights key details like involved areas of the brain, typical frequencies, symptoms, and potential treatments.