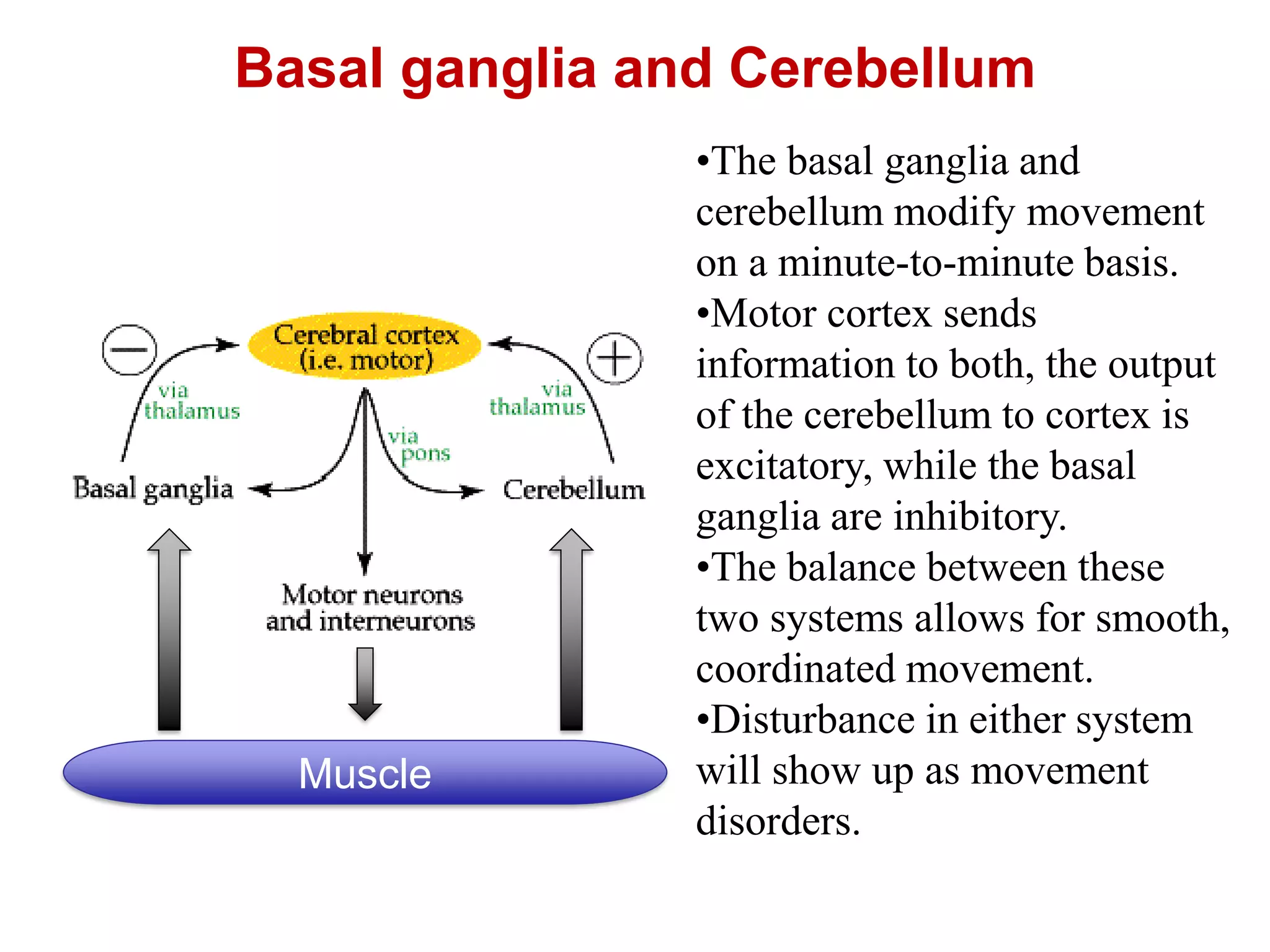
The document discusses the basal ganglia. It notes that the basal ganglia and cerebellum work together to modify movement on a minute by minute basis, with the basal ganglia being inhibitory and the cerebellum being excitatory. Disturbances in either system can cause movement disorders. The basal ganglia are composed of the striatum, globus pallidus, substantia nigra, and subthalamic nucleus. They receive input from the cortex and thalamus and output mainly to the thalamus. The basal ganglia help control voluntary movement, muscle tone, and are involved in arousal. Disorders like Parkinson's disease and chorea can result from basal ganglia dysfunction.