
![Vf AND ICP/MAP
• As long as MAP remains >70 mm of Hg,
increase of ICP [upto 20 mm of Hg] has no
major impact on Vƒ
• When MAP is significantly lowered → CBF↓
→ CPP↓, Vƒ↓](https://image.slidesharecdn.com/kaushalcsfphysiologypresentation-180405172422/85/CSF-physiology-18-320.jpg)
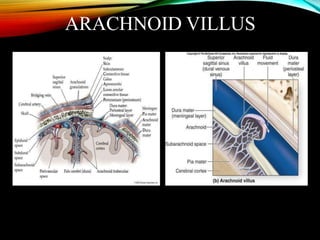
![CSF RESORPTION
• CSF is absorbed primarily by arachnoid villi
(granulations) that extend into the dural venous
sinuses.
• Arachnoid Villi are protrusion of the arachnoid matter
through perforations in the dura into the lumina of
venous sinuses
• Other sites of absorption include the choroid plexuses
and lymphatics.
• Intracranial-Superior sagittal sinus[85%-90%]
• Spinal-dural sinusoids on dorsal nerve roots[15%]](https://image.slidesharecdn.com/kaushalcsfphysiologypresentation-180405172422/85/CSF-physiology-19-320.jpg)
![MECHANISM OF CSF
REABSORPTION
• High velocity of blood flow through the fixed
diameter of the sinuses & the low intraluminal
pressure that develops @ the circumference of
the sinus wall where the arachnoid villi enter,
cause a suction –pump action
• Rate of reabsorption (Va); @ ICPs > 7 cms of
H2O, Va ↑ directly as ICP ↑[relation linear upto
ICP of 30 cms of H2O]](https://image.slidesharecdn.com/kaushalcsfphysiologypresentation-180405172422/85/CSF-physiology-21-320.jpg)
![DETERMINANTS OF
REABSORPTION
• Endothelium covering the villus acts as a CSF-
blood barrier
• If through endothelium:(1)pinocytic vesicles
(2)transcellular openings
• Trans villous hydrostatic pressure gradient [CSF
pressure-Venous sinus pressure]
• Resorption remains normal upto a CSF pressure
of 30 cm of H2O; above this it decreases](https://image.slidesharecdn.com/kaushalcsfphysiologypresentation-180405172422/85/CSF-physiology-22-320.jpg)
![METABOLIC REGULATION
HYPOTHERMIA: ↓ Vf – By decreasing
secretory and transport process and by ↓ing
CBF
between 41310 C: each 10 C↓in
temperature, ↓ Vf by 11%
HYPOCAPNIA: acutely ↓ Vf [mechanism :
↓ CBF, ↓ H+ for exchange with Na]](https://image.slidesharecdn.com/kaushalcsfphysiologypresentation-180405172422/85/CSF-physiology-34-320.jpg)
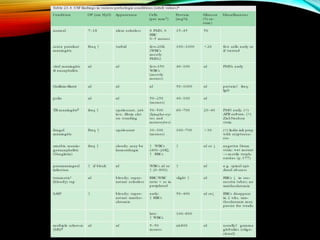


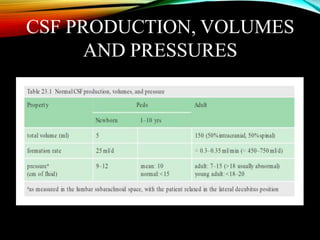
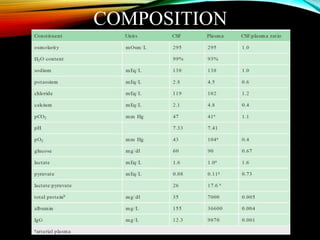
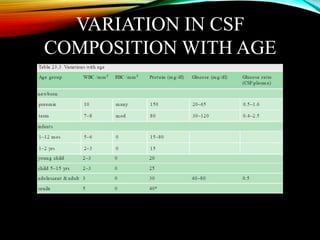
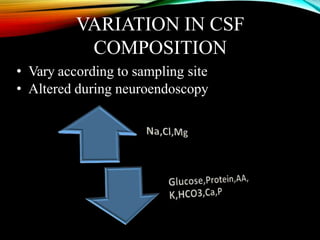
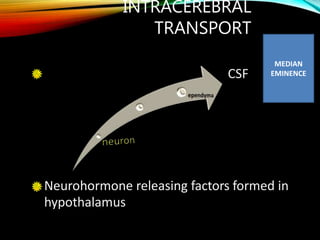
This document discusses cerebrospinal fluid (CSF) physiology and summarizes a presentation given by Dr. Kaushal Deep Singh. It outlines the history of CSF discovery. CSF is formed primarily by the choroid plexuses in the ventricles and circulates through the ventricles and subarachnoid spaces before being reabsorbed into the venous sinuses. The composition, circulation, and factors regulating CSF formation and reabsorption are described. Alterations in CSF dynamics can occur in various pathologies.























































































