ANATOMY AND PHYSIOLOGY
•Cerebrospinal fluid (CSF) is present within the subarachnoid
space surrounding the brain in the skull and the spinal cord
in the spinal column.
• It is a clear , colorless , transparent fluid present in the
cerebral ventricles, spinal canal and subarachnoid spaces.
• Formed mainly by choroid plexus
3.
Function of CSF
•_It's main function is to protect the brain and the spinal cord
from injury by acting as a fluid cushion.
• It is the medium through which nutrients and the waste
products are transported between brain/spinal
cord and the blood.
4.
Formation of CSF
•CSF is derived by ultra filtration of plasma and by secretion
through the choroid plexus located in the ventricles of the
brain.
• Reabsorbtion of CSF occurs at the arachnoid villi which
projects in the venous sinuses in the duramater.
• CSF is produce at the rate of 500 mL/day.
• Rate of formation – about 20ml/hr
5.
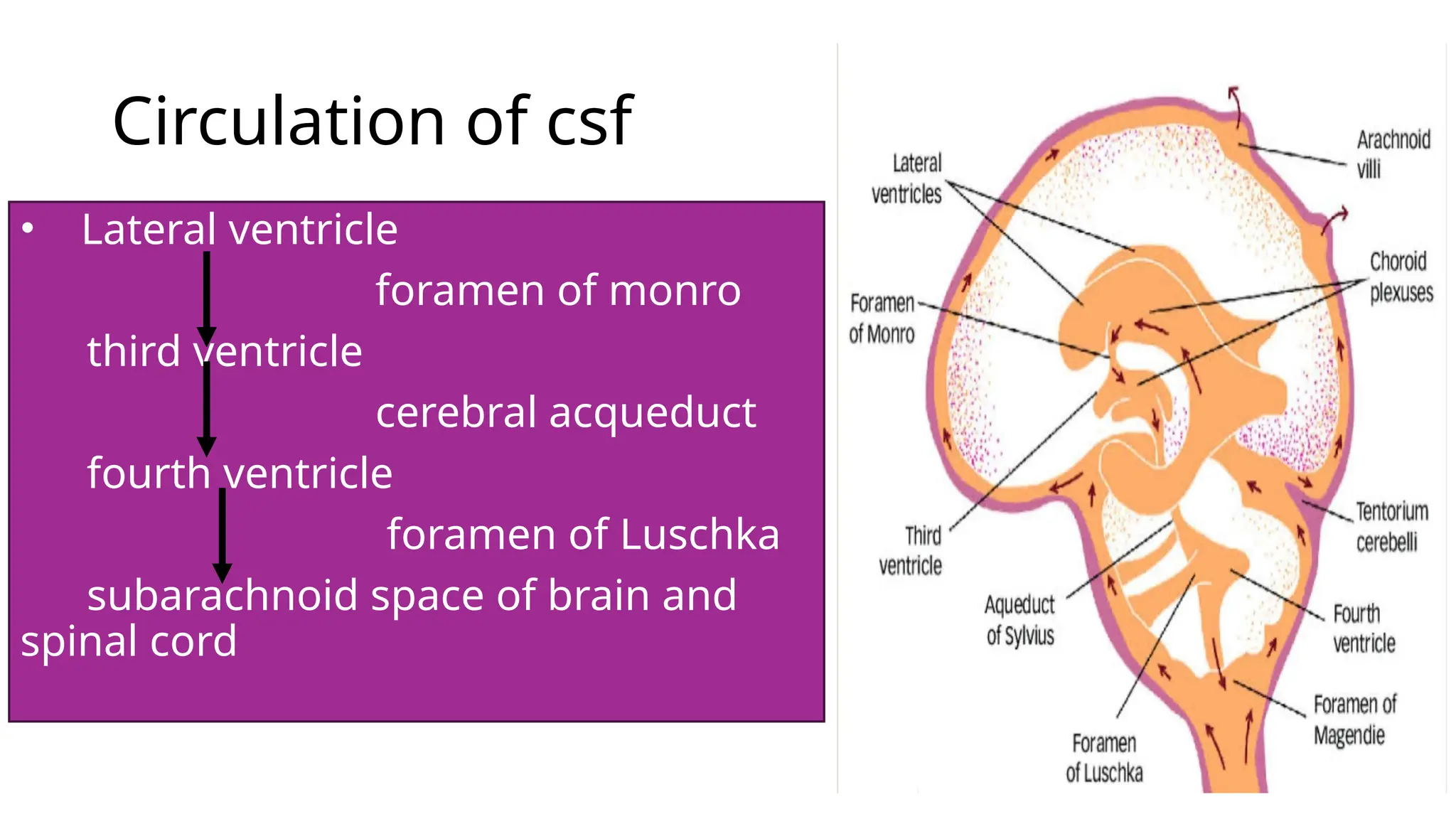
Circulation of csf
•Lateral ventricle
foramen of monro
third ventricle
cerebral acqueduct
fourth ventricle
foramen of Luschka
subarachnoid space of brain and
spinal cord
6.
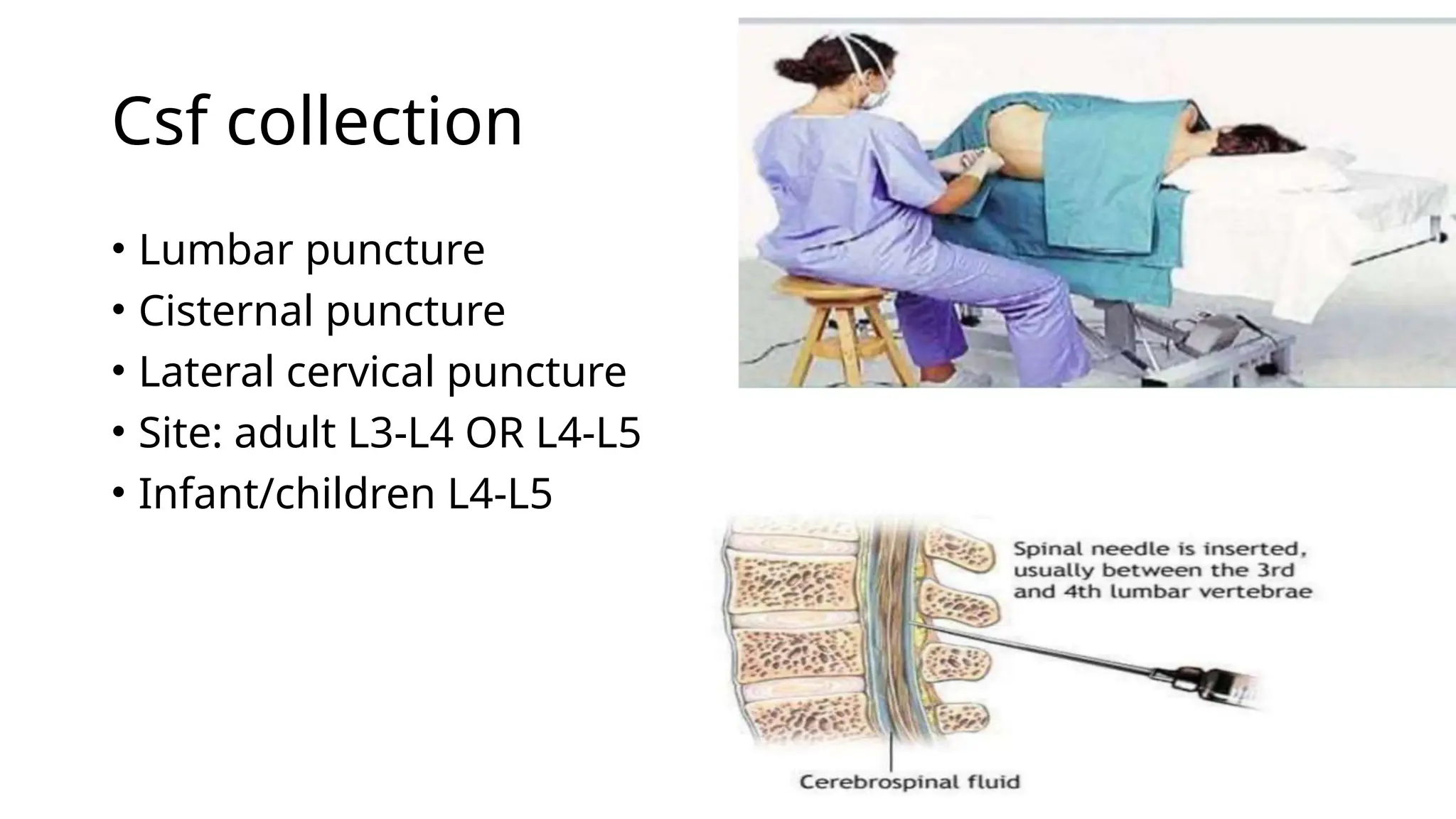
Indication of csfexamination
Diagnosis of suspected cases-
1) CNS Infections: Meningitis, Encephalitis
2) Inflammatory conditions: multiple sclerosis, Guillain bare
syndrome.
3) Infiltrative conditions: Leukemia, lymphoma
4) Administration of drug in CSF (therapeutic aim):
Antibiotics
Anticancer drugs
Anesthetic drugs
5)Introduction of radiographic contrast media for
myelograpghy.
7.
Complications of Lumbarpuncture
A)Post puncture headache (d/t leakage of csf)
B)Introduction of infection if aseptic precautions.
C)Herniation of brain
D) Dry tap (failure to obtain csf)
8.
Contraindication of lumbarpuncture
• Patient does not give consent.
• Raised intracranial pressure
• Skin infection at puncture.
• Coagulpathy/ bleeding disorder
• Any mass lesion at or above lumbar puncture site.
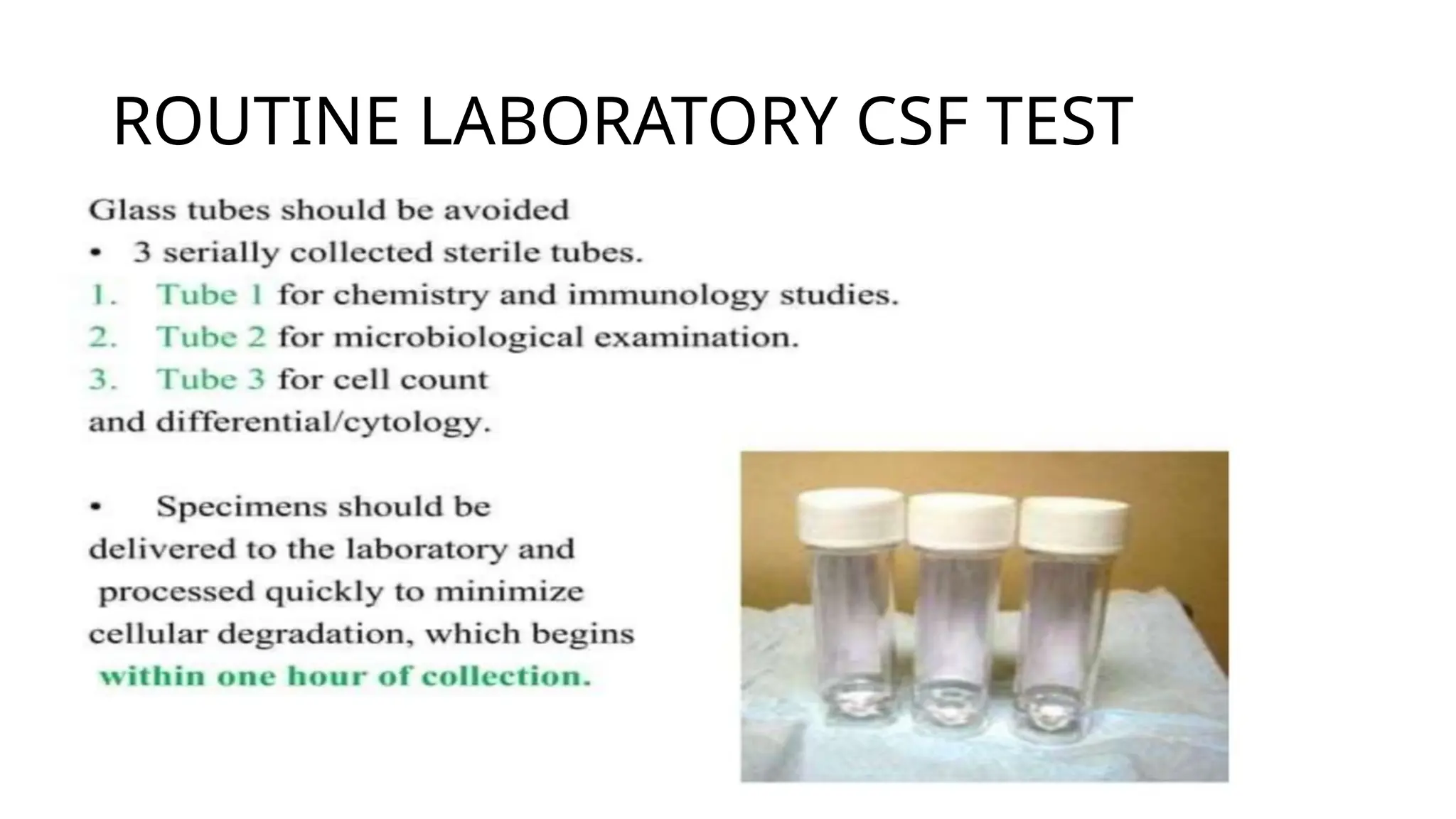
• After collectioncsf sample should be sent to lab
immediately, and examined without delay.
- Cells disintegrate rapidly
- Reduction of glucose (Glycolysis)
• Examined within 1 hour of collection .
• Specimen for bacterial culture should not be refrigerated,
because fastidious organism do not survive in cold
temperature.
DIFFERENTIAL CELL COUNT
•Preparation by centrifuge
• Other technique- cytocentrifuge, sedimentation , filtration
• Normally Lymphocytes and monocytes are present in small
numbers in a ratio of 70:30
• . Monocytes are more in number in neonates and children.