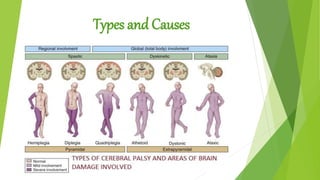
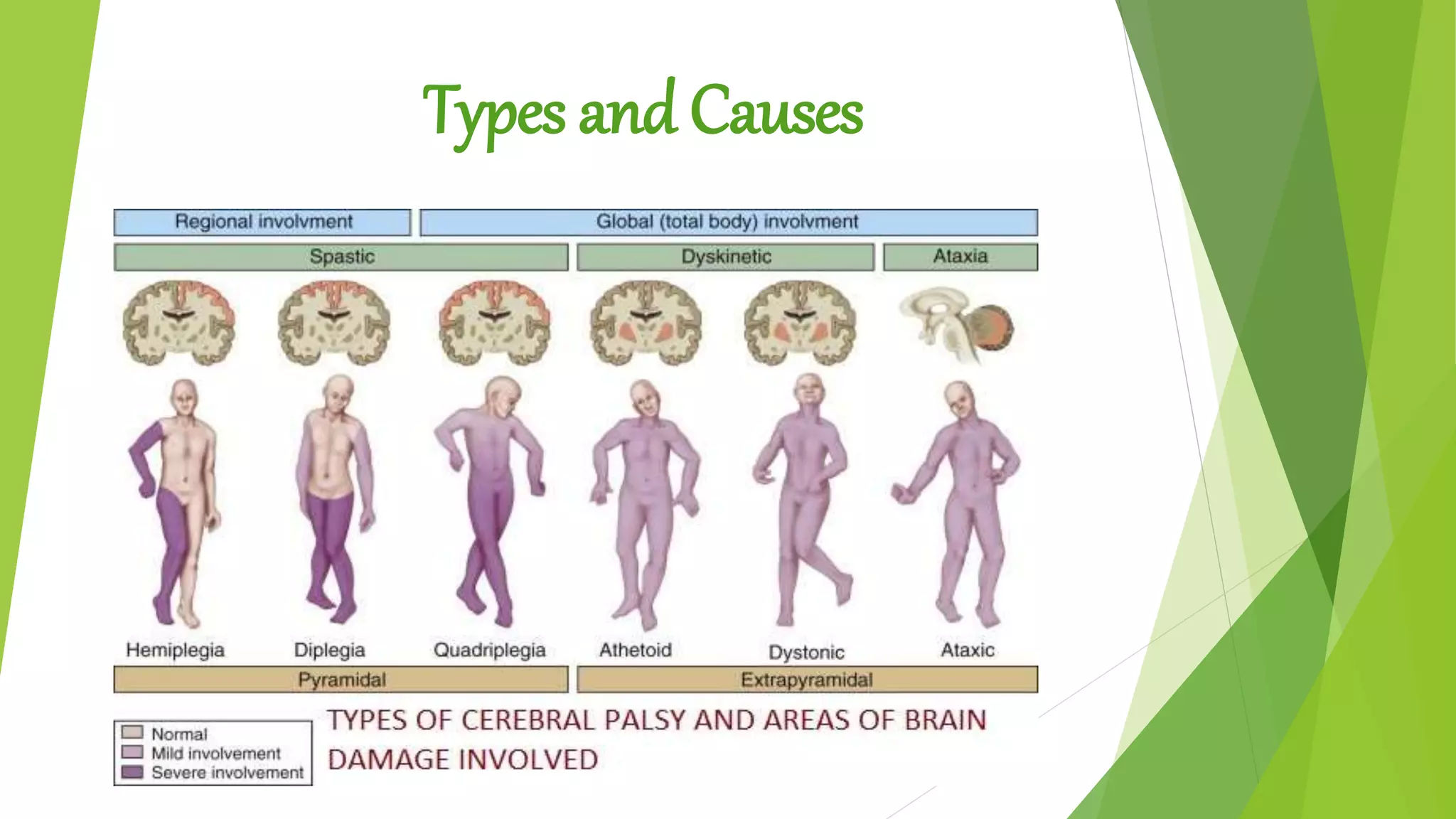
Cerebral palsy is caused by damage to the developing brain, which can occur during pregnancy, delivery, or early childhood. Over three quarters of cases result from issues during pregnancy, such as infection, lack of oxygen, prematurity, or genetic factors. Between 40-50% of cerebral palsy cases are in children born prematurely, with risks increasing the earlier the birth. Other risk factors include complications during delivery, low birth weight, infections, and genetic disorders. The main types of cerebral palsy are spastic, dyskinetic, ataxic, and mixed, defined by the pattern of muscle tone and movement abnormalities.