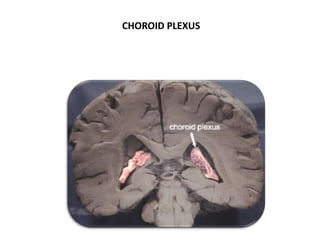
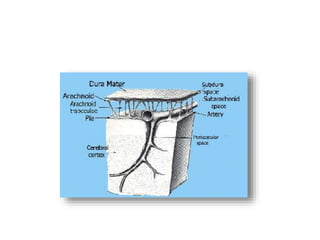
The document discusses hydrocephalus, including its evaluation, management, anatomy, physiology, and various classifications. It details cerebrospinal fluid (CSF) production, circulation, pressure, and types of hydrocephalus such as communicating and non-communicating. Additionally, it covers clinical features, diagnostic methods, and treatment options including drug therapy and surgical interventions like shunt placement.


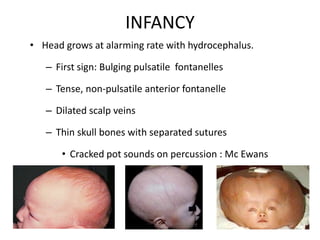






































































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

