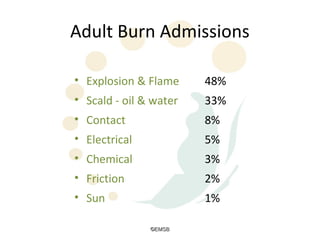
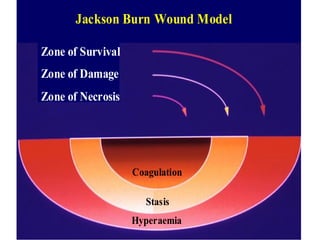
The document discusses emergency management of burns. It provides information on common causes of burns, pathophysiology involving initial and secondary tissue damage, burn wound classification models, and initial management following the EMSB (airway, breathing, circulation, disability, exposure, fluids) protocol. Key points include fluid resuscitation using the Parkland formula, monitoring for signs of circulatory obstruction in limbs, considering escharotomy if needed, and criteria for burn patient transfer to a specialized burn unit.






























































![5.2 Burn[1]](https://cdn.slidesharecdn.com/ss_thumbnails/52-burn1-1202268563653474-3-thumbnail.jpg?width=640&height=640&fit=bounds)





































