INTRO
Immediate care ofthe patient
Assessment of the burn wound
Fluid resuscitation
Additional aspects
Minor / outpatient wounds
Non-thermal burn injury
3.
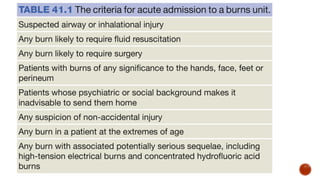
IMMEDIATE CARE OFTHE BURN PATIENT
Prehospital care
Ensure rescuer safety
Stop the burning process - Stop,drop and roll
Check for other injuries - standard ABC check followed by a rapid secondary survey
Cool the burn wound - minimum of 10 minutes - provides analgesia and slows the
delayed microvascular damage
Give oxygen - fire in an enclosed space - especially in altered consciousness
Elevate - life saving in case of delayed resuscitation,will reduce swelling and
discomfort in limbs.
4.
Hospital care
A, Airwaycontrol.
B,Breathing and ventilation.
C, Circulation.
D, Disability – neurological status.
E,Exposure with environmental control.
F,Fluid resuscitation.
Not all burn patients has to be admitted to a burns unit
6.
Airway
• The burnedairway swells - completely occlude the upper airway
• Secure the airway with an endotracheal tube until the swelling
has subsided
• Symptoms of laryngeal oedema - change in voice,stridor,anxiety
and respiratory difficulty
• Early Intubation of the suspected airway
• Should be ready to perform emergency cricothyroidotomy,if
intubation is delayed
7.
Recognition of thepotentially burned airway
A history of being trapped in the presence of smoke or hot gases
Burns on the palate or nasal mucosa, or loss of all the hairs in the
nose
Deep burns around the mouth and neck
8.
Breathing
Inhalational injury
Clinical features- progressive increase in respiratory effort and
rate,rising pulse, anxiety, confusion and decreasing oxygen
saturation
Physiotherapy, nebulisers and warm humidified oxygen are used.
If the situation deteriorates,give continuous or intermittent positive
pressure
Thermal burn injury to the lower airway
Rare
Treatment - supportive and same as in inhalational injury
9.
Metabolic poisoning
Clues- Historyof a fire within an enclosed space and any history of
altered consciousness
Blood gases must be measured immediately
Carboxyhaemoglobin levels raised above 10% - high inspired
oxygen for 24 hours
Mechanical block to breathing
Cause carbon dioxide retention and high inspiratory pressures if the
patient is ventilated.
Make scoring cuts through the burned skin to allow the chest to
expand (escharotomy).
10.
Assessing size
Thepatient’s whole hand is 1% TBSA - useful in small burns
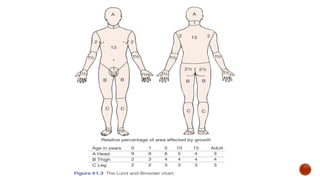
The Lund and Browder chart is useful in larger burns
The ‘rule of nines’ is adequate for a first approximation
Each upper limb is 9% TBSA
Each lower limb is 18%
Torso - 18% each side
Head and neck - 9%
ASSESSMENT OF THE BURN WOUND
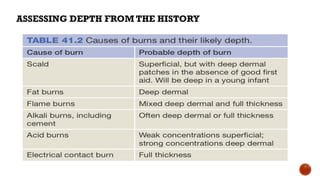
Burning ofhuman skin is temperature- and time dependent
It takes 6 hours for skin maintained at 44°C to suffer irreversible
changes
Surface temperature of 70°C for 1 s produce epidermal destruction.
Superficial partial-thickness burns
• no deeper than papillary dermis
• have capillary refilling
• heal without residual scar
• Treatment: non-surgical
14.
Deep partial-thicknessburns
do not blanch, but have some sensation
Damage deeper parts of reticular dermis
Reduced sensation
Lead to hypertrophic scarring
Full-thickness burns
feel leathery and have no sensation
Whole of dermis is destroyed
No capillary return
Completely anaesthetised
15.
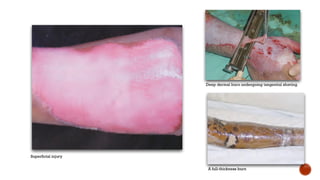
Deep dermal burnundergoing tangential shaving.
A full-thickness burn
Superficial injury
16.
FLUID RESUSCITATION
Principle:Intravascular volume must be maintained following
a burn to provide sufficient circulation to perfuse not only the
essential visceral organs but also the peripheral tissues.
In children with burns over 10% TBSA and adults with burns
over 15% TBSA, consider the need for intravenous fluid
resuscitation
If oral fluids are to be used,salt must be added
17.
3 types offluid used:
Ringer’s lactate
Human albumin solution or fresh frozen plasma
Hypertonic saline
Fluids needed can be calculated from Parkland’s formula -
This calculates the fluid to be replaced in the first 24 hours
Total percentage body surface area × weight (kg) × 4 =
volume (mL)
18.
CRYSTALLOID RESUSCITATION
• Mostcommonly used crystalloid-Ringer’s lactate
• Effective as colloids for maintaining intravascular volume
• Less expensive
• Maintenance fluid given in children
19.
HYPERTONIC SALINE
• Hyperosmolarityand hypernatremia
• Reduces shift of intracellular water to extracellular space
Advantages:
oLess tissue edema
oDecrease in escharotomies and intubations
20.
COLLOID RESUSCITATION
• Humanalbumin solution-common
• Plasma proteins cause inward oncotic pressure-counteracts
outward capillary osmotic pressure
• Given after first 12 hours of burn
Muir and Barclay formula:
• 0.5 x percentage BSA burnt x weight=one portion
• One portion given in each period
21.
Monitoring of resuscitation
Thekey is to monitor urine output
Urine output should be between 0.5 and 1.0 mL/kg body weight per
hour
If the urine output is below this, the infusion rate should be increased
by 50%
Measures of tissue perfusion such as acid–base balance are
appropriate in larger,more complex burns
22.
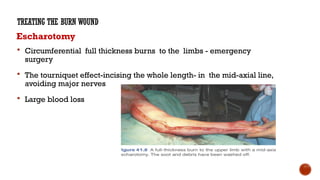
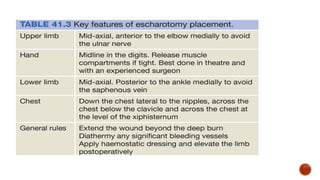
Escharotomy
Circumferential fullthickness burns to the limbs - emergency
surgery
The tourniquet effect-incising the whole length- in the mid-axial line,
avoiding major nerves
Large blood loss
TREATING THE BURN WOUND
24.
Full-thickness burns andobvious deep dermal wounds
Silver sulphadiazine cream (1%)
- broad spectrum prophylaxis against bacteria - Pseudomonas
aeruginosa and MRSA
Silver nitrate solution (0.5%)
- highly effective as a prophylaxis against pseudomonas
- not as active as silver sulphadiazine against some g-ve aerobs
- needs to be changed or the wounds resoaked every 2–4 hours
25.
Mafenide acetate cream
-5% topical solution
- painful to apply
- has been associated with metabolic acidosis
Silver sulphadiazine and cerium nitrate
- induces a sterile eschar on the burned skin
- reduce some of the cell-mediated immunosuppression that
occurs in burns
26.
Superficial partial-thickness woundsand mixed-
depth wounds
• Heal almost irrespective of the dressing
• The key lies with dressings (easy to apply,non painful,simple to
manage and locally available
• If contaminated,clean with a general anaesthetic and
sulphadiazine cream(chronic,for 2/3 days)
• Simplest method – exposure
• Exudate-frequent changes of linen
• Or permeable dressing-Mefix-avoid problems of wound
adherence
27.
• AVaseline-impregnated gauze/ a fenestrated silicone sheet
reduces the stiffness of the dry eschar, preventing it from
cracking
• More interactive dressings –Hydrocolloids(Duoderm) and
Biological dressings
need to change every 3-5 days
Provide moist envt-epithelialization
Mixed depth wounds
28.
• Biological ,synthetic(Biobrane), and natural(amniotic
membrane)
• also provide good healing envt,
• do not need to be changed ,
• ideal for superficial burns
• Early debridement and grafting –deep partial and full
thickness burns
• An optimal healing envt can make a difference to outcome in
borderline depth wounds
29.
ADDITIONAL ASPECTS OFTREATING THE BURNED PATIENT
Analgesia
Acute
Small burns - oral analgesics - paracetamol and NSAIDs
Topical cooling
Large burns - IV opiates
IM injections should not be given in acute burns over 10% of TBSA - absorption is
unpredictable and dangerous.
Subacute
Large burns,continuous analgesia - begin with infusions,continue with oral tablets ( slow
release morphine )
Powerful,short-acting analgesia - before dressing changes
30.
Energy balance andnutrition
Burn - > 15% TBSA in adults and >10% in children - additional
nutrition needed
A nasogastric tube should be used in all patients with burns
over 15% of TBSA
Removing the burn and achieving healing stops the catabolic
drive
32.
MONITORING AND CONTROLOF INFECTION
Patients with major burns are immunocompromised
Large portals of entry-pathogenic and
opportunistic bacteria and fungi
Compromised local defences in the lung
and gut –edema
Monitoring lines and catheters
Proper hand washing and other cross contamination prevention
measures are required
Monitored through-bacteriological surveillance,catheter tips , sputum
33.
• If thereare signs of infection –culture-antibiotics started
• Signifacant temp –above 38.5 c
• Significant rise /fall in wbc count ,thrombocytosis, increasing
signs of catabolism
• Intense nursing care
• Physiotherapy
• Psychological support –post traumatic reactions
34.
SURGERY FOR THEACUTE BURN WOUND
• Any deep partial- thickness and full thickness burns except those are <4cm2 need surgery
• Indeterminate depth –reassessed after 48 hours
• Deep dermal burns need tangential shaving and split-skin
• Grafting
• The anaesthetist needs to be ready for significant blood loss
• Topical adrenaline (1:1 000 000 or 1:500 000) reduces bleeding
• All burnt tissue needs to be excised
• Stable cover,permanent or temporary,should be applied at once to reduce burn load
35.
Delayed reconstruction andscar management
• Eyelids must be treated before exposure keratitis arises
• Early intervention contracture causing signi loss of range of
movement of a joint
• Burn alopecia is best treated with tissue expansion of the
unburned hair-bearing skin
• Transposition flaps and Z-plasties with or without tissue
expansion are useful
• Full-thickness grafts and free flaps may be needed for large or
difficult areas
• Hypertrophy is treated with pressure garments
• Pharmacological treatment of itch is important
36.
MINOR BURNS/OUTPATIENT BURNS
Localburn wound care
Blisters
Arguments -
Blister fluid depresses immune function, slowing down chemotaxis
and intracellular killing and also acting as a medium for bacterial
growth
Leaving blisters intact as they form a sterile stratum spongiosum
Leaving a ruptured blister is not advised.
Initial cleaning of the burn wound -Wash the burn with chlorhexidine
37.
Topical agents
Initial managementof minor burns - superficial or partial thickness
- dressings with a non-adherent material -Vaseline-impregnated
gauze or Mepitel
(5 days )
- by definition,should be healed after 7–10 days
Silver sulphadiazine (1%) or Flamazine is the most commonly used
topical agent - avoided in pregnant women,nursing mothers and
infants less than 2 months of age (risk of kernicterus)
38.
Dressing the minorburn wound
• Dressing - decrease wound pain,protect and isolate the burn wound
• Small superficial burn -Vaseline gauze or another non-adherent dressing - first
layer - gauze or Kerlix - second layer - don’t impede the circulation
• Bulkiness of dressings depends upon the amount of wound discharge
Synthetic burn wound dressings - popular
Decrease pain associated with dressings
Improve healing times
Decrease outpatient appointments
Lower overall costs
39.
Healing of burnwounds
Burns - managed conservatively - healed in 3 weeks.If no signs of re-epithelialisation - debridement and grafting
Infection
Managed using a combination of topical and systemic agents.
Debridement and skin grafting should also be considered.
Itching
Histamine and endopeptides cause itching
Antihistamines, analgesics, moisturising creams, aloe vera, antibiotics, gabapentin, cyproheptadine, loratidine
and topical doxepin cream.
Traumatic blisters
Coz of new fragile epithelium
Moisturiser and non adherent dressings will suffice
40.
NON-THERMAL BURN INJURY
Electricalinjuries
Divided into low- and high- voltage injuries,the threshold being 1000 v
Low-voltage injuries cause small,localised,deep burns
They can cause cardiac arrest through pacing interruption without significant direct
myocardial damage
High-voltage injuries damage by flash (external burn) and conduction (internal burn)
Myocardium may be directly damaged without pacing interruption
Limbs may need fasciotomies or amputation
Look for and treat acidosis and myoglobinuria
41.
An exit woundof a high-tension injury, with a dead big toe and significant damage to the medial portion of
the second toe.
Amputation and cover with the lateral portion of the second toe.
42.
Chemical injuries
• Damageis from corrosion and poisoning
• Copious lavage with water helps in most cases
• Then identify the chemical and assess the risks of absorption
• Common cause of acid burns is hydrofluoric acid - initial
management is with calcium gluconate gel topically
• When burnt with a concentration greater than 50% - threat of
hypocalcaemia and subsequent arrhythmias - indication for acute
early excision.
43.
Ionising radiation injury
Localburns causing ulceration need excision and vascularised
flap cover, usually with free flaps
Systemic overdose needs supportive treatment
44.
Cold injuries
Two types:acute cold injuries from industrial accidents and frostbite
The tissue is more resistant to cold injury than to heat injury -
inflammatory reaction is not as marked
Affect the peripheries in cold climates
The initial treatment is with rapid rewarming in a bath at 42°C
Produce delayed microvascular damage similar to that of cardiac
reperfusion injury
Management - mainly conservative