This document discusses burns, including their classification, pathophysiology, management, and special considerations for inhalation injuries and airway management. Some key points include:
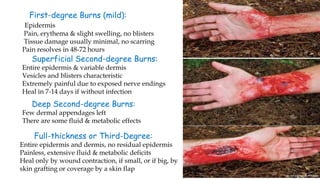
- Burns are classified by depth and total body surface area affected. Deep second and third-degree burns require grafting or flaps for healing.
- Burns cause local tissue damage and systemic inflammatory responses impacting circulation, immunity, metabolism, and other organ systems.
- Initial management focuses on airway protection, fluid resuscitation, pain control and wound care. Admission criteria include burns over 15% of total body surface area or those involving special areas.
- Inhalation injuries are suspected with certain histories and symptoms and require early intubation