Downloaded 53 times
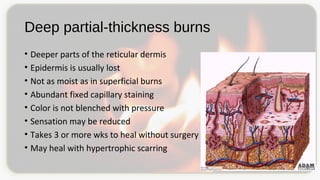
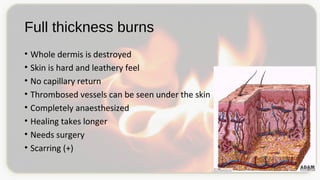
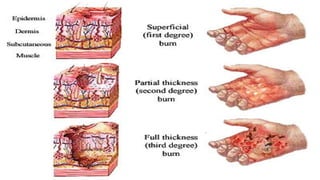



This document discusses types and degrees of burns, including thermal, electrical, chemical, and radiation burns. It describes the anatomy of the skin and degrees of burn damage from superficial to full thickness. Treatment approaches are outlined, including immediate care, fluid resuscitation based on percentage of total body surface area burned, wound treatment techniques, surgery, reconstruction, and complications. The focus is on clinical assessment and management of burn patients.


















































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


