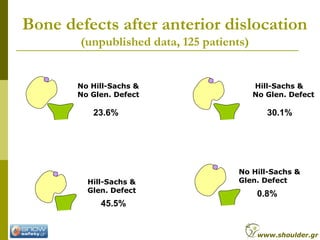
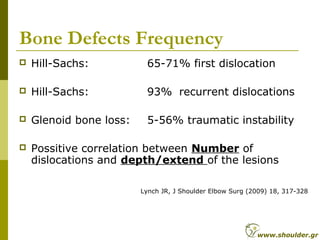
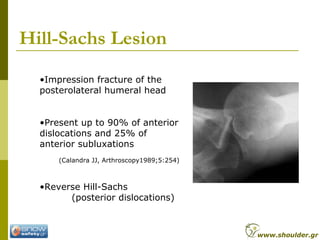
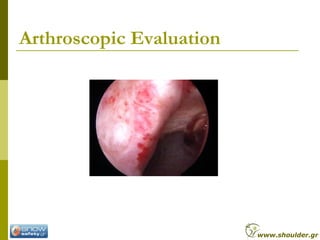
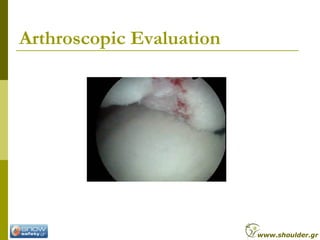
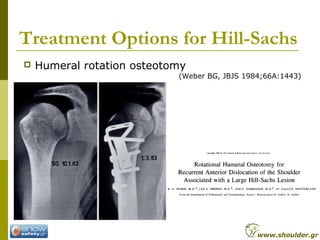
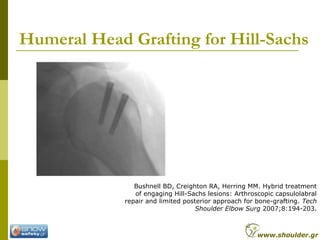
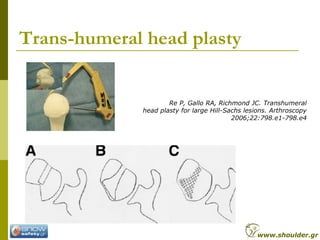
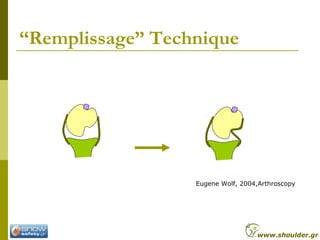
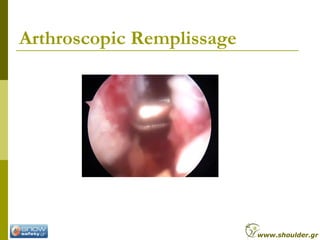
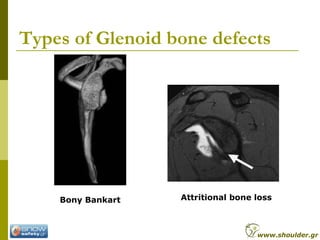
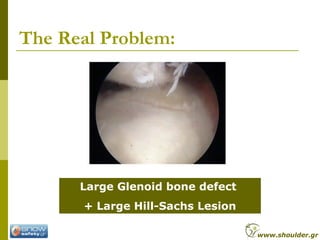
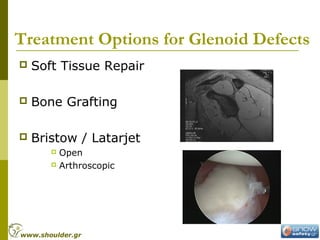
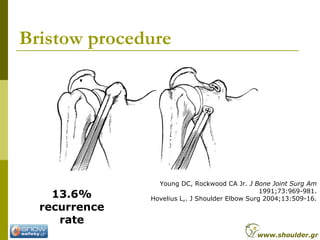
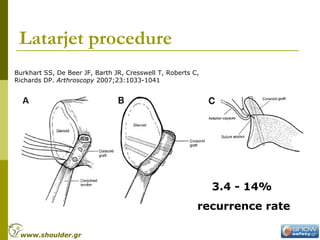
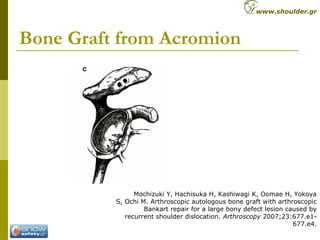
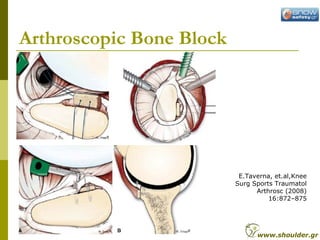
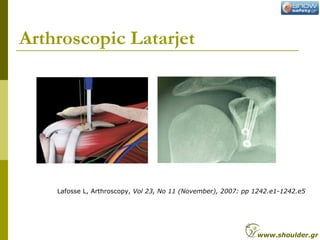
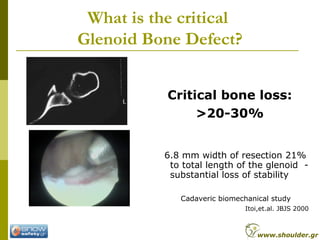
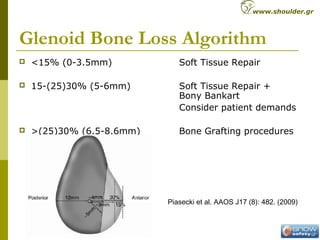
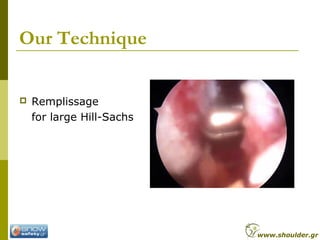
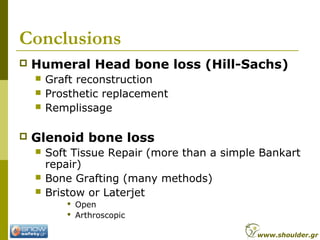
This document discusses treatment options for bone defects in the glenoid and humeral head that can cause recurrent shoulder instability. It finds that humeral head (Hill-Sachs) defects occur in 65-93% of cases depending on the number of dislocations, while glenoid defects occur in 5-56% of cases. Treatment depends on the size and engagement of the defects. For large Hill-Sachs lesions, options include bone grafting, arthroplasty, or the remplissage procedure. For significant glenoid bone loss over 20-30%, options include soft tissue repair plus bone grafting or procedures like Bristow or Latarjet to add bone to the glenoid. The document advocates
![Hemi-CAP
Raiss P, Aldinger PR, Kasten P, Rickert M, Loew M. Humeral
head resurfacing for fixed anterior glenohumeral dislocation.
Int Orthop 2007 Dec 19 [Epub ahead of print]
www.shoulder.gr](https://image.slidesharecdn.com/8lrzfolvqparnjigoyft-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100657/85/Bone-defects-thessal2010-19-320.jpg)
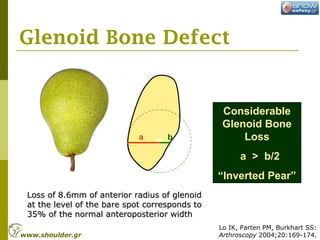
![Background Knowledge
Considerable Glenoid defects
after shoulder dislocation
decrease the intrinsic
stability.
[Burkhart, De Beer, Itoi, Mologne]
In vitro, less forces need to
dislocate the shoulder.
[Burkhart SS. Arthroscopy, 2000]
www.shoulder.gr](https://image.slidesharecdn.com/8lrzfolvqparnjigoyft-signature-69d9f1a3cb3f2649714837b93c1c3b7b41f9a67bbef005eecf911e10fcb33758-poli-170927100657/85/Bone-defects-thessal2010-23-320.jpg)































































































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)














